






No concern generates more anxiety in TRT consultations — and more reflexive clinical refusals — than prostate health. The belief that testosterone feeds prostate cancer, that TRT will cause the prostate to grow out of control, and that PSA will inevitably rise to dangerous levels are deeply embedded in both lay and medical thinking. Many men are told by their GPs that they cannot have TRT and Prostate Health because of their prostate history, their PSA level, or simply their age.
At Vitalis Luxe Clinic in Hull, we take prostate health seriously. It is part of every TRT assessment and every monitoring programme. But we also take our responsibility to present accurate, current evidence seriously — and the evidence on testosterone and prostate health has changed substantially over the past two decades, in ways that have not always been reflected in standard clinical practice.
This article explains the actual relationship between testosterone and the prostate, what the evidence shows about TRT and prostate cancer risk, what PSA monitoring means in the context of TRT, and what conditions genuinely represent contraindications versus those that have been overstated as risks.
Table of Contents
The Historical Fear: Where It Came From

The belief that testosterone promotes prostate cancer derives primarily from observations made in the 1940s by Charles Huggins, who showed that castration (removal of the primary testosterone source) caused regression of metastatic prostate cancer — work for which he received the Nobel Prize in 1966. The logical inference drawn from this observation — that if removing testosterone shrank prostate cancer, then adding testosterone must promote it — became medical orthodoxy for decades.
This inference was reasonable based on what was known at the time. But subsequent decades of research have substantially complicated the picture, and the simple ‘more testosterone = more prostate cancer’ model is no longer supported by the evidence as it was once understood.
The Androgen Saturation Model: Why More Testosterone Is Not Proportionally More Risk
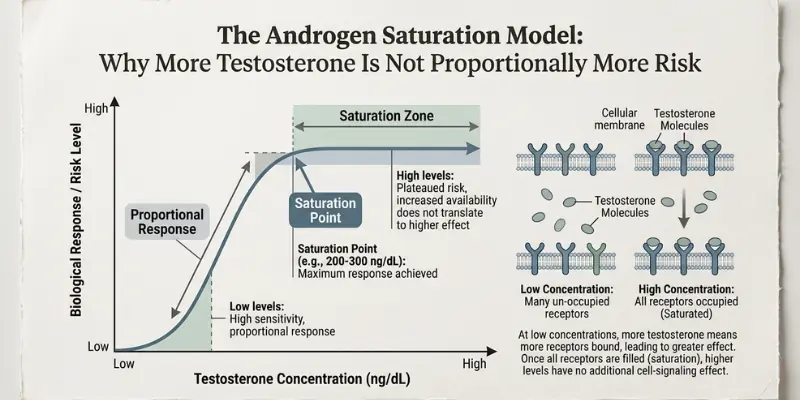
The key conceptual shift is the androgen saturation model, developed from research by Abraham Morgentaler and others. The model proposes that prostate androgen receptors become saturated at relatively low testosterone levels — meaning that once testosterone exceeds a threshold concentration (estimated at approximately 8 nmol/L, well within the hypogonadal range), additional testosterone has little or no additional stimulatory effect on prostate tissue.
The evidence supporting this model is compelling. Large epidemiological studies find no correlation between higher testosterone levels and prostate cancer risk in the normal physiological range. Men with the highest testosterone levels do not have higher rates of prostate cancer than men with average levels. And critically: men with the lowest testosterone levels — hypogonadal men — do not have lower rates of prostate cancer than eugonadal men. If testosterone were linearly promoting prostate cancer, the opposite would be expected in both cases.
Studies administering Testosterone Replacement Therapy to hypogonadal men find that PSA rises modestly in the first 3–6 months — predominantly reflecting restoration of normal prostate function rather than pathological growth — and then stabilises. It does not continue to rise indefinitely. Prostate volume similarly stabilises after an initial modest increase. This is exactly what the saturation model predicts: the prostate responds to testosterone restoration up to the saturation point, then plateaus.
The Clinical Bottom Line on TRT and Prostate Cancer Current evidence does not support the conclusion that TRT in hypogonadal men significantly increases the risk of developing prostate cancer beyond baseline population risk. Multiple large systematic reviews and meta-analyses have failed to demonstrate a causal relationship between TRT and prostate cancer incidence. TRT may be associated with the detection of pre-existing subclinical prostate cancer — through increased PSA surveillance — rather than the promotion of new cancer. This is not the same as causing cancer. |
PSA: What It Measures and What It Means on TRT

Prostate-specific antigen (PSA) is a glycoprotein produced by prostate epithelial cells and secreted into semen. A small amount leaks into the bloodstream and is measurable by a blood test. Elevated PSA is associated with several prostate conditions — benign prostatic hyperplasia (BPH), prostatitis, and prostate cancer — but is not specific to cancer. Most men with elevated PSA do not have prostate cancer.
How TRT Affects PSA

In hypogonadal men starting TRT, PSA typically rises in the first 3–6 months as the prostate adjusts to restored testosterone levels. This rise is generally modest — usually 0.5–1.0 ng/mL in most men — and stabilises thereafter. A PSA rise within this range during the initial treatment period is a normal, expected response, not a warning sign of cancer.
However, a rapid or disproportionate PSA rise on TRT — particularly a rise above 1.4 ng/mL within 12 months of starting treatment, or any result above 4.0 ng/mL (or above 3.0 ng/mL in higher-risk men) — warrants urological assessment. This is why PSA is measured at baseline before starting TRT and at each monitoring visit thereafter.
PSA Monitoring Protocol at Vitalis Luxe Clinic
- Baseline PSA before any TRT is commenced — this is mandatory and non-negotiable; PSA cannot be meaningfully interpreted on TRT without a pre-treatment baseline
- PSA at 3–6 months — initial response assessment; confirms the PSA is rising within expected limits
- PSA at 12 months — stability confirmation
- Annual PSA thereafter — ongoing monitoring throughout treatment
- Any PSA result above threshold or showing an unexpected rapid rise triggers urological referral before continuing TRT
Important: Finasteride and PSA

Men who are also taking finasteride (for hair loss) alongside TRT should be aware that finasteride reduces PSA by approximately 50%. A PSA of 1.5 ng/mL on finasteride should be doubled to 3.0 ng/mL for interpretation purposes. Failure to account for this can produce a falsely reassuring PSA result. At Vitalis Luxe Clinic, all PSA results on finasteride are interpreted with this correction applied.
Benign Prostatic Hyperplasia: A Separate Consideration
Benign prostatic hyperplasia (BPH) — non-cancerous enlargement of the prostate — is extremely common in men over 50. BPH is androgen-dependent, and testosterone does contribute to prostate growth, though the saturation model applies here too — the prostate growth response to TRT plateaus rather than progressing indefinitely. The concern with BPH and TRT is not cancer risk but lower urinary tract symptoms (LUTS) — urinary frequency, urgency, poor stream, and nocturia — which may worsen if the prostate enlarges further.
For men with significant pre-existing BPH symptoms, TRT requires careful consideration and close monitoring for LUTS worsening. It is not an absolute contraindication — many men with well-managed BPH receive TRT without meaningful symptom deterioration — but it requires a clinical discussion about the risk-benefit balance and a clear monitoring plan.
Medications used to treat BPH — 5-alpha reductase inhibitors (finasteride, dutasteride) and alpha-blockers — are compatible with TRT and may provide partial protection against TRT-related BPH worsening. Men on dutasteride for BPH may find that it also addresses hair loss concerns — an incidental benefit.
When TRT Is Genuinely Contraindicated Due to Prostate Concerns
Some prostate-related situations represent genuine contraindications to TRT, at least in the short term:
- Active or suspected prostate cancer — TRT is contraindicated in men with known untreated prostate cancer; the androgen saturation model does not override the risk in already-established malignant disease. Men in whom prostate cancer has been definitively treated and who have achieved sustained undetectable PSA may be candidates for TRT under specialist oncological guidance — this is an evolving area
- PSA above 4.0 ng/mL (or 3.0 ng/mL in high-risk men) without urological evaluation — TRT should not be started until elevated PSA has been investigated and malignancy excluded
- Rapid recent PSA rise without investigation — a PSA velocity above 0.75 ng/mL per year warrants urological assessment before TRT initiation
- Metastatic prostate cancer — TRT is contraindicated; androgen deprivation therapy, not testosterone supplementation, is the standard hormonal approach in metastatic disease
The important distinction: having a history of prostate cancer that has been treated and monitored to remission is not necessarily a permanent contraindication to TRT. This is an area of active clinical research. Selected men with treated, non-metastatic prostate cancer who have achieved prolonged remission have received TRT under specialist supervision in published case series without adverse prostate outcomes. This is a specialist discussion — not a decision made in a general TRT clinic — but it should not be dismissed without a nuanced clinical assessment.
Practical Pre-TRT Prostate Assessment at Vitalis Luxe Clinic
Assessment Component | Why It Matters | Action if Abnormal |
|---|---|---|
PSA blood test (baseline) | Establishes the pre-treatment reference point; cannot interpret on-treatment PSA without baseline | If elevated (>3–4 ng/mL depending on age/risk), urological assessment before starting TRT |
Digital rectal examination (DRE) | If elevated (>3–4 ng/mL, depending on age/risk), urological assessment before starting TRT | If abnormal, urological referral regardless of PSA result |
Lower urinary tract symptoms (LUTS) history | Identifies significant pre-existing BPH that may worsen with TRT | If significant LUTS: detailed risk-benefit discussion; possibly specialist urology input before TRT |
Family history of prostate cancer | First-degree relative with prostate cancer increases individual risk; informs PSA threshold for action | Lower action threshold for PSA (3.0 ng/mL rather than 4.0 ng/mL); closer monitoring |
Age | Baseline prostate cancer risk increases with age; PSA interpretation is age-adjusted | Age-appropriate PSA thresholds applied |
Ethnicity | Men of Black African/Caribbean descent have approximately 2.5x higher prostate cancer risk | Lower PSA action threshold; earlier monitoring; explicit family history discussion |
Frequently Asked Questions
Does TRT cause prostate cancer?
Current evidence does not support the conclusion that TRT in hypogonadal men significantly increases prostate cancer risk beyond baseline population risk. The androgen saturation model explains why: prostate androgen receptors saturate at low testosterone levels, meaning that restoring testosterone from deficient to normal ranges does not produce proportional increases in prostate cell stimulation. Multiple systematic reviews and meta-analyses have failed to demonstrate a causal relationship between TRT and prostate cancer incidence.
Will TRT make my PSA go up?
PSA typically rises modestly in the first 3–6 months of TRT as the prostate adjusts to restored testosterone — a normal physiological response. This rise is usually 0.5–1.0 ng/mL and stabilises thereafter. It does not continue to rise indefinitely. Pre-treatment PSA baseline is mandatory at Vitalis Luxe Clinic, and PSA is monitored at 3–6 months, 12 months, and annually thereafter. Any unexpected or disproportionate rise triggers a urological assessment.
Can I have TRT if my PSA is slightly elevated?
A PSA above the age-appropriate threshold (typically 3.0–4.0 ng/mL) requires urological assessment before TRT is started — not necessarily TRT refusal. If urological assessment finds no evidence of malignancy and identifies a benign cause (BPH, prostatitis), TRT may proceed with appropriate monitoring. TRT should not begin while elevated PSA is uninvestigated. At Vitalis Luxe Clinic, PSA above threshold results in urology referral and TRT deferral pending investigation.
I’ve had prostate cancer — can I ever have TRT?
This is an evolving area. Traditional guidance treats any prostate cancer history as a permanent contraindication to TRT. More recent evidence from specialist centres suggests that selected men with treated, non-metastatic prostate cancer who have achieved sustained remission (undetectable PSA after treatment) may receive TRT without adverse prostate outcomes, under specialist oncological supervision. This is not a decision for a general TRT clinic — it requires specialist prostate oncology input. Active or metastatic prostate cancer remains a contraindication.
What is the androgen saturation model?
The androgen saturation model proposes that prostate androgen receptors become saturated at low testosterone concentrations — approximately 8 nmol/L, well within the hypogonadal range. Once saturation is reached, additional testosterone has little further stimulatory effect on prostate tissue. This explains why men with the highest physiological testosterone levels do not have higher prostate cancer rates, and why restoring testosterone from deficient to normal levels does not produce proportional prostate cancer risk increases.
Does testosterone make BPH worse?
TRT may modestly increase prostate volume in men with BPH, potentially worsening lower urinary tract symptoms (urinary frequency, urgency, poor stream). This risk is manageable — prostate growth plateaus rather than progressing indefinitely, and LUTS worsening is not universal. Men with significant pre-existing BPH symptoms should discuss this risk explicitly with their clinician before starting TRT. 5-alpha reductase inhibitors (finasteride, dutasteride) used for BPH may also provide partial protection against TRT-related prostate growth.
How often should PSA be checked on TRT?
At Vitalis Luxe Clinic: baseline before treatment; at 3–6 months; at 12 months; and annually thereafter. Any result above the age-appropriate threshold or any PSA velocity (rate of rise) above 0.75 ng/mL per year triggers urological referral. PSA monitoring is one of the most important safety components of any TRT programme and should never be omitted.
Where can I get a prostate assessment alongside TRT in Hull or Yorkshire?
Vitalis Luxe Clinic in Hull performs baseline PSA and clinical prostate assessment as a mandatory component of every TRT evaluation. We monitor PSA throughout treatment, apply age- and risk-appropriate thresholds, and refer to urology promptly where indicated. We serve men across Hull, East Yorkshire, and throughout Yorkshire — in person or online with home blood testing for most follow-up monitoring.