





The thyroid gland and the testicular HPG axis are the two most clinically significant hormonal systems affecting male energy, mood, body composition, and sexual function. They operate independently — but they interact in ways that clinicians and patients alike frequently overlook. A man with fatigue, low libido, and poor body composition may have testosterone deficiency, hypothyroidism, or both — and treating only one while ignoring the other produces incomplete results.
At Vitalis Luxe Clinic , thyroid function testing is included in our extended hormone assessment for men who present with fatigue and low-energy symptoms, because the symptom overlap between hypothyroidism and testosterone deficiency is substantial and the two conditions frequently co-occur. This article explains the relationship between thyroid hormones and testosterone, how to distinguish their effects, and why comprehensive hormonal assessment matters.
The Thyroid’s Role in Male Health
The thyroid gland produces two primary hormones: thyroxine (T4) and triiodothyronine (T3). T4 is the storage form — produced in large quantities and converted to the active T3 in peripheral tissues. T3 is the biologically active form that enters cells and regulates metabolic rate, protein synthesis, energy production, cardiac function, thermogenesis, mood, and cognitive speed. Virtually every cell in the body has thyroid hormone receptors — making thyroid hormone one of the most pervasive regulators of human physiology.
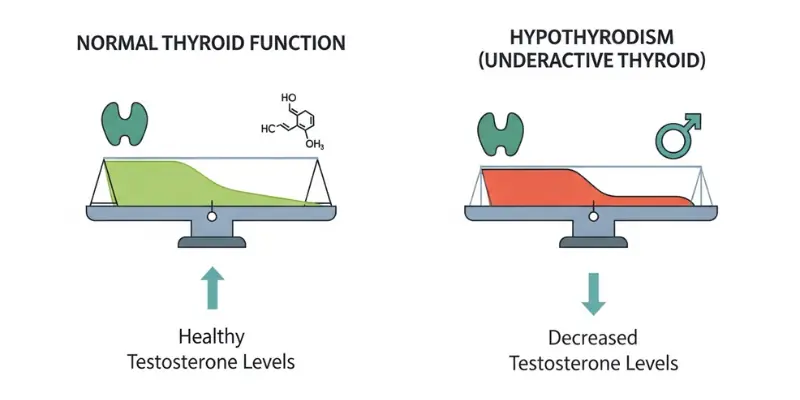
Hypothyroidism — insufficient thyroid hormone — is more common than generally recognised, with subclinical hypothyroidism (elevated TSH with normal T4) affecting approximately 5–10% of the adult population. Men are less frequently affected than women but are significantly under-screened. Because hypothyroidism produces profound metabolic slowing, its clinical effects — fatigue, weight gain, cold intolerance, slowed cognition, low mood, dry skin, and reduced libido — overlap substantially with the symptom picture of testosterone deficiency.
How Thyroid Hormones Affect Testosterone
SHBG Modulation

One of the most clinically important testosterone-thyroid interactions is through sex hormone-binding globulin (SHBG). Both hypothyroidism and hyperthyroidism alter SHBG levels — and since SHBG determines how much total testosterone is biologically active (free), changes in SHBG from thyroid dysfunction directly affect androgen status:
- Hypothyroidism reduces SHBG — appearing to improve free testosterone availability but potentially masking a genuinely low total testosterone; the net effect depends on the degree of SHBG suppression versus total testosterone reduction
- Hyperthyroidism increases SHBG — binding more testosterone and reducing free testosterone; men with hyperthyroidism may have apparently normal total testosterone but significantly reduced bioavailable testosterone
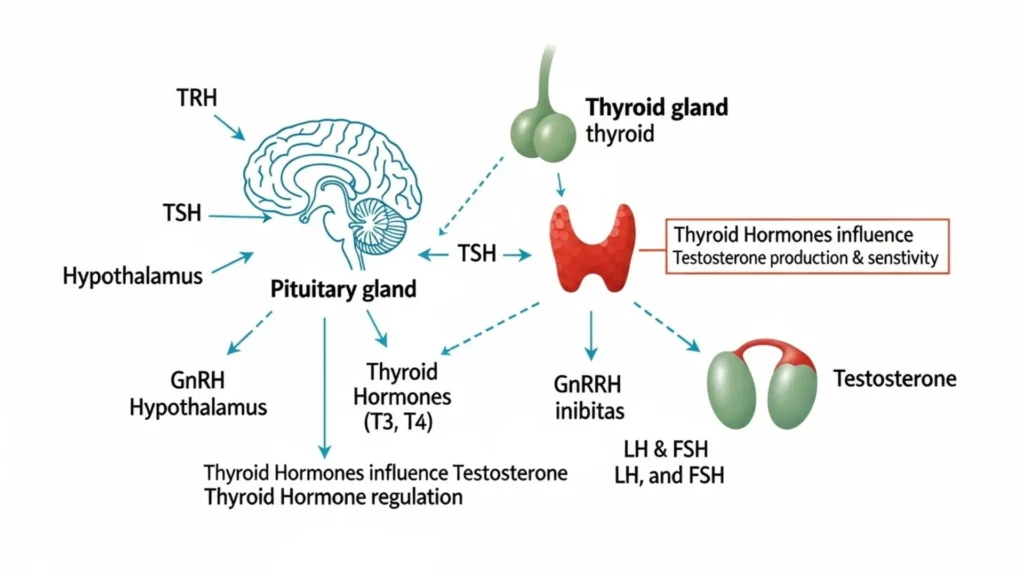
Direct HPG Axis Effects
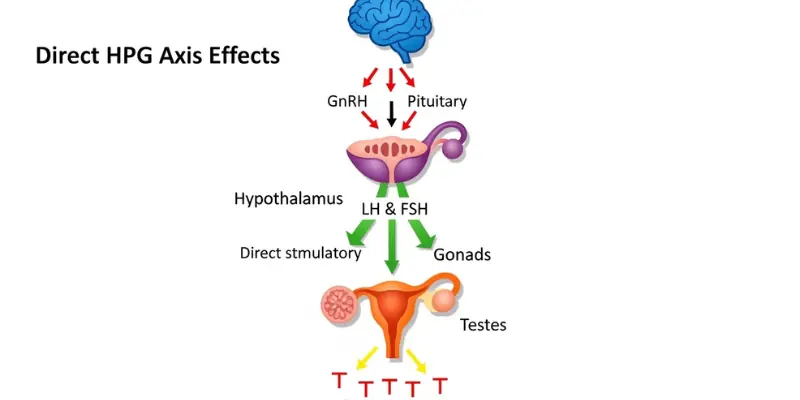
Thyroid hormones have direct effects on the HPG axis at multiple levels. Hypothyroidism can alter GnRH pulsatility and LH secretion, reducing the pituitary stimulus to testicular testosterone production. In men with severe hypothyroidism, total testosterone may be meaningfully reduced through this mechanism — restoring thyroid function with levothyroxine treatment can partially restore testosterone independently.
Leydig Cell Function
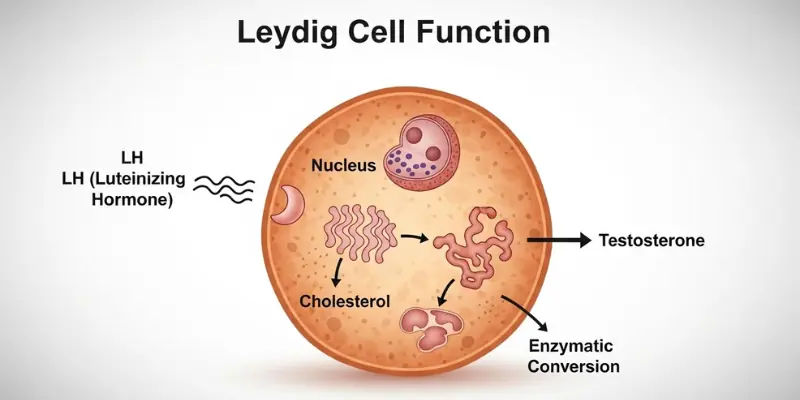
Thyroid hormone receptors are present on testicular Leydig cells, and thyroid hormones directly modulate Leydig cell steroidogenic capacity. Hypothyroidism impairs Leydig cell function — reducing testosterone production from the same LH stimulation that would produce more testosterone in a euthyroid man. This is a direct testicular effect, operating independently of the HPG axis modulation described above.
Prolactin
Severe hypothyroidism causes elevation of TRH (thyrotropin-releasing hormone) — which also stimulates prolactin release from the pituitary. Elevated prolactin directly suppresses the HPG axis, reducing LH/FSH and testosterone. A man with significant hypothyroidism may have both directly impaired testicular function and HPG axis suppression via prolactin elevation — a compound mechanism for testosterone reduction.
Symptom Overlap: How to Distinguish Hypothyroidism from Testosterone Deficiency
Symptom | Hypothyroidism | Testosterone Deficiency | Both |
|---|---|---|---|
Fatigue | Profound, constant, often worse in morning — ‘lead in the limbs’ | Significant but often more variable; energy may fluctuate | Both cause significant fatigue; combined presentation compounds severity |
Low libido | Present — reduced but typically not as pronounced as testosterone deficiency | Often the most prominent symptom; particularly absent spontaneous desire | Both reduce libido; testosterone deficiency typically produces more specific absence of desire |
Weight gain / difficulty losing weight | Characteristic — often significant central weight gain despite unchanged diet | Visceral fat accumulation; muscle loss; poor response to diet and training | Both cause body composition deterioration |
Cold intolerance / feeling cold | Characteristic of hypothyroidism — feeling cold when others are comfortable | Not characteristic | Cold intolerance strongly suggests thyroid component |
Low mood / depression | Common — often profound emotional flatness | Common — particularly irritability, low motivation, loss of drive | Both; clinical assessment needed to distinguish primary cause |
Cognitive slowing / brain fog | Often described as ‘thinking through treacle’ | Present but typically less severe | Both impair cognition; severe slowing suggests thyroid component |
Dry skin / hair loss | Characteristic — dry coarse skin, hair thinning, loss of outer eyebrow | Hair loss from DHT/androgenic alopecia — pattern different | Different hair loss patterns; dry skin more specific to hypothyroidism |
Erectile dysfunction | Can occur through vascular and neurological mechanisms | Very common through central desire reduction and vascular effects | Both contribute; addressing both needed for full recovery |
Morning erections | Reduced | Often significantly reduced or absent — highly characteristic | Both reduce; testosterone deficiency effect typically more pronounced |
Slow heart rate / constipation | Characteristic hypothyroidism signs | Not characteristic | These signs, if present, strongly suggest hypothyroidism |
The Clinical Approach: What to Test
At Vitalis Luxe Clinic, when men present with significant fatigue and multi-domain symptoms, our assessment extends beyond testosterone to include thyroid function — because incomplete hormonal assessment produces incomplete clinical conclusions. The minimum thyroid assessment for symptomatic men is:
- TSH (thyroid-stimulating hormone) — the primary screening test; elevated TSH indicates the pituitary is working hard to stimulate an underperforming thyroid; the most sensitive marker of primary hypothyroidism
- Free T4 — confirms whether the thyroid is actually producing adequate hormone in response to TSH stimulation
- Free T3 — the active hormone; some men have normal T4 but inadequate T3 conversion — the conversion is performed in peripheral tissues and can be impaired independently of thyroid production
- Thyroid antibodies (TPO and TG antibodies) — identify autoimmune thyroiditis (Hashimoto’s disease), the most common cause of hypothyroidism; important for predicting progression in subclinical disease
Interpreting results: TSH above 4.5 mU/L on two separate tests in a symptomatic man warrants treatment discussion. TSH 2.5–4.5 mU/L with symptoms is subclinical — monitoring and symptom tracking are appropriate; some symptomatic men in this range benefit from treatment. TSH below 0.4 mU/L suggests hyperthyroidism or excessive thyroid hormone. Free T3 in the lower quarter of the reference range in a symptomatic man may indicate impaired T4-to-T3 conversion — a clinically underrecognised scenario.
Treating Hypothyroidism Alongside Testosterone Deficiency
For men with both confirmed hypothyroidism and testosterone deficiency, thyroid treatment should typically be optimised first, or at minimum concurrent with TRT assessment — because restoring thyroid function may partially improve testosterone levels through the HPG axis and Leydig cell mechanisms described above. This is not always sufficient to resolve testosterone deficiency independently, but it is important to establish thyroid-replete status before making a definitive testosterone treatment decision.
Levothyroxine (synthetic T4) is the standard hypothyroidism treatment. Optimal dosing achieves TSH in the lower half of the reference range (0.5–2.0 mU/L) with normal free T4 — not simply TSH within the wide reference range. Some patients with persistent symptoms despite optimal T4 replacement benefit from the addition of liothyronine (T3 supplementation) where T4-to-T3 conversion is impaired — this is a specialist clinical decision.
Frequently Asked Questions
Can hypothyroidism cause low testosterone?
Yes — hypothyroidism impairs testosterone production through multiple mechanisms: reduced Leydig cell steroidogenic capacity (thyroid hormone receptors on Leydig cells modulate testosterone production); HPG axis disruption from altered GnRH pulsatility; and, in severe cases, elevated prolactin from TRH elevation, which directly suppresses LH/FSH. The effect varies in magnitude — mild hypothyroidism may have minimal direct testosterone impact; severe hypothyroidism can meaningfully reduce testosterone levels.
Do the symptoms of hypothyroidism and low testosterone overlap?
Substantially — fatigue, low libido, low mood, weight gain, cognitive slowing, and reduced exercise tolerance are shared symptoms of both conditions. Distinguishing features of hypothyroidism include cold intolerance, dry/coarse skin, hair thinning (including outer eyebrow loss), constipation, and bradycardia. These are not characteristic of testosterone deficiency. The most reliable distinguishing approach is blood testing — TSH for thyroid and testosterone (morning, fasting) for androgen status.
Should thyroid be tested alongside testosterone?
Yes — in men presenting with significant fatigue, low libido, and multi-domain symptoms, thyroid function testing should accompany testosterone assessment. Testing testosterone alone in a symptomatic man risks attributing all symptoms to androgen deficiency when hypothyroidism is the primary or contributing cause, resulting in TRT that provides incomplete benefit. At Vitalis Luxe Clinic, thyroid function is part of our extended assessment for men with unexplained fatigue and hormonal symptom clusters.
Can TRT help if I have hypothyroidism?
If you have both confirmed hypothyroidism and confirmed testosterone deficiency, both conditions warrant treatment — one does not preclude the other. TRT is not contraindicated in men with hypothyroidism, and levothyroxine is not contraindicated in men on TRT. Treating both conditions simultaneously addresses the full hormonal deficit rather than leaving one untreated. Thyroid optimisation should ideally precede or accompany TRT assessment, as thyroid restoration may partially improve testosterone levels.
Does TRT affect thyroid function?
TRT has modest effects on thyroid parameters. Testosterone affects SHBG, and thyroid hormones (particularly T4) are partly bound to transport proteins. TRT may modestly alter thyroid hormone transport — but these effects are generally not clinically significant in men with normal thyroid function on TRT. If thyroid symptoms develop or change after starting TRT, thyroid function re-testing is appropriate.
What is Hashimoto’s thyroiditis?
Hashimoto’s thyroiditis is an autoimmune condition in which antibodies attack the thyroid gland, causing progressive inflammation and functional decline leading to hypothyroidism over time. It is the most common cause of primary hypothyroidism. Thyroid peroxidase (TPO) and thyroglobulin antibodies are elevated. Men with subclinical hypothyroidism (elevated TSH, normal T4) and positive antibodies have high likelihood of progressing to overt hypothyroidism and benefit from closer monitoring and earlier treatment consideration.
Where can I get thyroid and testosterone testing in Hull or Yorkshire?
Vitalis Luxe Clinic in Hull includes thyroid function testing as part of our extended hormone panel for men with significant fatigue and multi-domain symptoms. If your symptoms have not been fully explained by testosterone assessment alone, or if you have never had thyroid function tested alongside testosterone, we can provide comprehensive hormonal assessment in person in Hull or with home blood testing across Yorkshire.