






The relationship between testosterone and metabolic health is one of the most clinically significant — and most underappreciated — in men’s medicine. At Vitalis Luxe Clinic in Hull, we regularly assess men who present with testosterone deficiency alongside type 2 diabetes, insulin resistance, or metabolic syndrome. This highlights the critical link between Testosterone and Diabetes, an area that is often overlooked in routine care. In many cases, these men have been managing their blood sugar for years without anyone asking whether their hormonal health might be contributing to it.
This is not a peripheral concern. Low testosterone and type 2 diabetes are so closely intertwined that each is both a cause and a consequence of the other. Men with testosterone deficiency are significantly more likely to develop insulin resistance and type 2 diabetes. Men with type 2 diabetes are significantly more likely to have low testosterone. The two conditions share underlying mechanisms and amplify each other in a self-reinforcing cycle that is genuinely difficult to break without addressing both dimensions.
In this article, we explain the mechanisms behind this relationship, what the evidence shows about TRT’s effects on metabolic parameters, how we approach this in clinical practice at our Hull clinic, and what men with diabetes or metabolic syndrome need to know before discussing TRT.
Table of Contents
The Bidirectional Relationship: Mechanism by Mechanism

How Low Testosterone Promotes Insulin Resistance and Diabetes
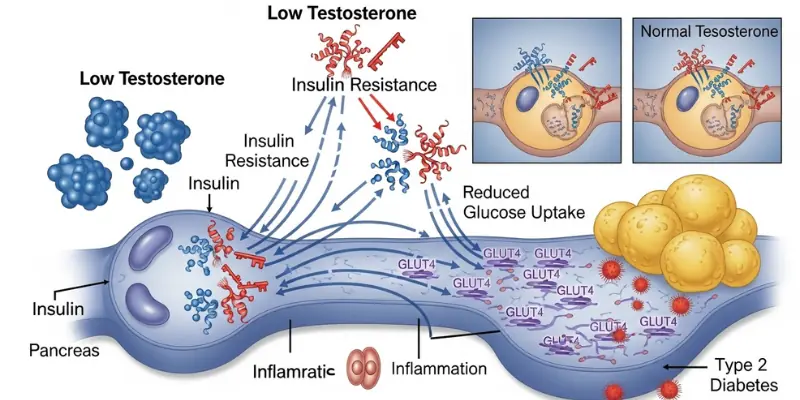
Testosterone plays a direct role in glucose metabolism through several well-characterised mechanisms. When it is deficient, these mechanisms fail — progressively shifting the metabolic environment toward insulin resistance and, ultimately, type 2 diabetes:
- Reduced skeletal muscle mass — testosterone is the primary anabolic driver of lean muscle tissue. Muscle is the largest site of glucose disposal in the body — approximately 80% of post-meal glucose uptake occurs in skeletal muscle. When testosterone deficiency causes muscle loss (sarcopenia), this disposal capacity is reduced, meaning glucose remains elevated in the bloodstream for longer after meals
- Increased visceral adiposity — as covered in our blog on testosterone and weight loss, testosterone deficiency promotes accumulation of visceral (abdominal) fat. Visceral fat is metabolically active, secreting adipokines and free fatty acids that directly impair insulin signalling in muscle and liver
- Direct impairment of insulin signalling — testosterone acts through androgen receptors on muscle and fat cells to enhance insulin receptor expression and glucose transporter (GLUT4) activity. Deficiency reduces both, impairing the cellular machinery that moves glucose from blood into cells
- Increased systemic inflammation — testosterone deficiency is associated with elevated CRP and inflammatory cytokines (IL-6, TNF-alpha). Chronic low-grade inflammation directly impairs insulin signalling through inflammatory kinase pathways (IKK-beta, JNK)
- Impaired pancreatic beta-cell function — androgen receptors are present on pancreatic beta cells; some evidence suggests testosterone directly supports insulin secretory capacity
The cumulative effect of these mechanisms: testosterone deficiency creates a metabolic environment characterised by reduced glucose disposal, increased insulin resistance, compensatory hyperinsulinaemia, and progressive beta-cell stress — the classic pathway to type 2 diabetes. Men with testosterone deficiency have approximately 2.4 times the risk of developing type 2 diabetes compared to eugonadal men in large epidemiological studies.
How Type 2 Diabetes and Insulin Resistance Suppress Testosterone

The reverse pathway is equally well-established. Type 2 diabetes and insulin resistance suppress testosterone through multiple routes:
- HPG axis disruption — insulin resistance and hyperinsulinaemia alter hypothalamic GnRH pulsatility, reducing LH and FSH secretion and therefore testicular stimulation. The pituitary becomes less responsive to GnRH stimulation in metabolic syndrome
- Elevated oestradiol from aromatase — the visceral fat accumulation that accompanies insulin resistance and diabetes contains high aromatase activity, converting testosterone to oestradiol and further suppressing HPG axis feedback
- Reduced SHBG — insulin resistance directly suppresses hepatic SHBG production. This creates the paradox of apparently normal total testosterone with significantly reduced free testosterone, as SHBG falls. While low SHBG appears to ‘free up’ testosterone, the simultaneous reduction in testicular production means the net effect is often reduced androgen activity
- Direct Leydig cell impairment — oxidative stress and advanced glycation end-products (AGEs) associated with chronic hyperglycaemia appear to directly impair Leydig cell steroidogenesis
- Obesity-related leptin resistance — leptin, produced by fat cells, has complex effects on the HPG axis; leptin resistance in obese men with type 2 diabetes disrupts hypothalamic hormonal signalling
The result: more diabetes = less testosterone = more diabetes. This cycle compounds over years and explains why men with long-standing, poorly controlled type 2 diabetes often have severely suppressed testosterone — and why addressing the hormonal dimension cannot be separated from addressing the metabolic one.
Metabolic Syndrome: The Common Ground

Between testosterone deficiency and type 2 diabetes sits metabolic syndrome — a cluster of metabolic abnormalities that dramatically increase the risk of both type 2 diabetes and cardiovascular disease. Metabolic syndrome is defined by the presence of three or more of:
- Central obesity — waist circumference above 102cm in men (94cm by some European criteria)
- Elevated triglycerides — above 1.7 mmol/L
- Reduced HDL cholesterol — below 1.0 mmol/L in men
- Elevated blood pressure — above 130/85 mmHg or on antihypertensive treatment
- Elevated fasting glucose — above 5.6 mmol/L or on glucose-lowering treatment
Testosterone deficiency is strongly and independently associated with metabolic syndrome — the prevalence of low testosterone in men with metabolic syndrome is approximately double that of men without it. And the relationship is bidirectional: each component of metabolic syndrome contributes to testosterone suppression, while testosterone deficiency contributes to each component of metabolic syndrome.
This means that for men presenting with metabolic syndrome, testosterone assessment is not an optional extra it is a clinically essential part of understanding the hormonal dimension of what is driving their metabolic picture.
What TRT Does for Metabolic Parameters: The Evidence
Effects on Insulin Sensitivity and HbA1c
Multiple randomised controlled trials and meta-analyses have examined the effects of TRT on insulin resistance and glycaemic control in hypogonadal men with type 2 diabetes or metabolic syndrome. The consistent findings:
- TRT significantly reduces HbA1c (glycated haemoglobin — the primary marker of long-term blood glucose control) in hypogonadal men with type 2 diabetes — reductions of 0.3–0.5% HbA1c are clinically meaningful and consistent across trials
- TRT improves insulin sensitivity (HOMA-IR) in hypogonadal men — the metabolic mechanism involves both direct insulin receptor enhancement and secondary improvements through body composition change
- TRT reduces fasting glucose in men with metabolic syndrome and testosterone deficiency
- The TIMES2 study (a UK multicentre randomised controlled trial) demonstrated that TRT significantly improved insulin resistance, glycaemic control, and dyslipidaemia in hypogonadal men with type 2 diabetes and metabolic syndrome — one of the most clinically relevant TRT trials for this patient group
Effects on Body Composition in Diabetic Men
The body composition improvements of TRT — reduced visceral fat, increased lean muscle mass — are particularly relevant for diabetic men, because the mechanisms that drive these changes are the same mechanisms that improve insulin sensitivity. As visceral fat reduces, aromatase activity falls, the HPG axis feedback normalises, and both testosterone and metabolic parameters improve together.
Effects on Lipid Profile
TRT has a complex and variable effect on lipid profile — total cholesterol and LDL may modestly reduce in some studies, while HDL (the ‘protective’ cholesterol) may also reduce slightly. The overall lipid impact of TRT in the context of metabolic syndrome is generally neutral to mildly beneficial, particularly when combined with the body composition improvements that reduce atherogenic dyslipidaemia more substantially than TRT alone.
TRT in Diabetic Men: Clinical Considerations
Is TRT Safe with Diabetes?
TRT is not contraindicated in men with type 2 diabetes — in fact, the evidence suggests it may be beneficial for their metabolic control. However, several clinical considerations apply:
- Diabetes medications may need review as insulin sensitivity improves on TRT men on sulphonylureas or insulin who develop improved glucose control may require dose reduction to avoid hypoglycaemia; coordination with the diabetes team or GP is appropriate
- Haematocrit monitoring is particularly important — men with diabetes may already have elevated cardiovascular risk, and erythrocytosis from TRT requires careful management in this population
- Blood pressure should be monitored closely — hypertension is common in metabolic syndrome and requires attention alongside TRT
- Regular HbA1c tracking alongside standard TRT monitoring allows the metabolic benefit to be documented and medication adjusted appropriately
Realistic Expectations
TRT is a meaningful component of metabolic management in hypogonadal men with type 2 diabetes — but it is not a standalone treatment for diabetes. The most effective approach combines TRT with sustained lifestyle intervention: progressive resistance training (which improves insulin sensitivity through muscle glucose disposal), dietary management, adequate sleep, and stress reduction. TRT enables the lifestyle work to be more effective by restoring the hormonal environment in which muscle can be built, energy is available for exercise, and motivation is restored.
Men who start TRT without making lifestyle changes may see modest metabolic improvements but will not achieve the transformative metabolic outcomes possible when TRT is combined with consistent training and dietary management. The combination is synergistic.
| Metabolic Parameter | Effect of Low T | Effect of TRT in Hypogonadal Men | Timeline for Improvement |
|---|---|---|---|
| HbA1c | Elevated — sustained hyperglycaemia in deficient men | Significantly reduced in trials of hypogonadal diabetic men — clinically meaningful reductions | 3–6 months of treatment |
| Fasting Glucose | Elevated — impaired fasting glucose common in deficiency | Reduced in metabolic syndrome studies | 2–4 months |
| Insulin Resistance (HOMA-IR) | Substantially elevated | Improved — both direct and indirect (via body composition) mechanisms | 3–6 months |
| Visceral Fat | Increased — promotes insulin resistance | Progressively reduced with sustained TRT | 6–12 months (with lifestyle) |
| Lean Muscle Mass | Reduced — impairs glucose disposal | Increased with exercise — restores primary glucose disposal site | 3–12 months (with training) |
| Triglycerides | Elevated — atherogenic dyslipidaemia pattern | Moderately reduced | 3–6 months |
| HDL Cholesterol | Reduced | Variable — modest reduction in some studies, improvement with weight loss | Variable |
| Blood Pressure | Often elevated (metabolic syndrome) | Modest improvement in some studies — body composition changes help | 6–12 months |
Frequently Asked Questions
Does low testosterone cause type 2 diabetes?
Low testosterone is strongly associated with increased risk of type 2 diabetes — epidemiological studies find approximately 2–2.5 times the diabetes risk in hypogonadal men compared to those with normal testosterone. The mechanisms are direct: reduced muscle mass impairs glucose disposal, increased visceral fat promotes insulin resistance, and testosterone deficiency directly impairs insulin receptor signalling. The relationship is bidirectional diabetes also suppresses testosterone, creating a self-reinforcing metabolic-hormonal cycle.
Can TRT improve blood sugar control in diabetic men?
Yes — in hypogonadal men with type 2 diabetes, TRT consistently improves HbA1c, fasting glucose, and insulin resistance in clinical trials. The UK TIMES2 trial demonstrated significant improvements in insulin resistance and glycaemic control with TRT in this patient group. The magnitude of improvement is clinically meaningful and comparable to some glucose-lowering medications. TRT works best for metabolic control when combined with exercise and dietary management.
Will I need to change my diabetes medication if I start TRT?
Potentially — as insulin sensitivity improves on TRT, men on sulphonylureas (such as gliclazide) or insulin may experience improved glycaemic control that requires dose reduction to prevent hypoglycaemia. This should be managed in coordination with whoever prescribes your diabetes medications. At Vitalis Luxe Clinic, we recommend informing your diabetes team or GP when starting TRT so that monitoring and medication review can be appropriately arranged.
What is metabolic syndrome and how does it relate to testosterone?
Metabolic syndrome is a cluster of metabolic risk factors — central obesity, elevated triglycerides, low HDL, elevated blood pressure, and elevated fasting glucose — that dramatically increases cardiovascular and diabetes risk. Testosterone deficiency is strongly and independently associated with metabolic syndrome, approximately doubling its prevalence. Each component of metabolic syndrome contributes to testosterone suppression, while testosterone deficiency worsens each component. The two conditions are deeply intertwined and both benefit from the same intervention: lifestyle optimisation alongside hormonal correction where testosterone is deficient.
Can losing weight raise testosterone without TRT in diabetic men?
Significant weight loss — particularly visceral fat reduction — can meaningfully raise testosterone in overweight men with type 2 diabetes whose testosterone is low-normal rather than severely deficient. Reducing visceral fat decreases aromatase activity, improves insulin sensitivity, and can partially restore HPG axis function. For men with severely deficient testosterone from primary or secondary hypogonadism, weight loss alone is unlikely to fully restore levels. The clinical approach depends on the degree of deficiency and the individual’s metabolic context.
Is TRT safe if I have diabetic kidney disease or complications?
Men with significant diabetic complications — including nephropathy, neuropathy, or severe retinopathy — require careful clinical assessment before TRT. Haematocrit elevation from TRT is particularly important to manage carefully in men with cardiovascular risk from diabetes complications. This does not mean TRT is contraindicated — the metabolic benefits may be substantial — but it means closer monitoring and coordination with relevant specialists. At Vitalis Luxe Clinic, we take a comprehensive view of each patient’s clinical picture before recommending a treatment approach.