





One of the most common situations that brings men to Vitalis Luxe Clinic in Hull is not that they haven’t considered their symptoms — it’s that they have already been to their GP, had their testosterone tested, and been told that treatment isn’t available to them on the NHS. Sometimes they are told their levels are ‘normal for their age.’ Sometimes they are told the NHS doesn’t fund TRT for their presentation. Sometimes they are simply given a leaflet and advised to exercise more.
The NHS access landscape for testosterone replacement therapy in England — and specifically in Yorkshire — is genuinely complicated. What is available varies by ICB (Integrated Care Board), by GP practice, and sometimes by individual GP. The clinical thresholds applied vary. The willingness to refer varies. And the waiting times for specialist endocrinology review, where referral is made, can be substantial.
This article explains how NHS TRT access actually works in Yorkshire, why men are frequently declined treatment despite genuine clinical need, what private Getting TRT on the NHS offers that the NHS typically does not, how shared care arrangements work, and what men need to know to navigate the system effectively — whichever route they choose.
Table of Contents
How NHS TRT Access Works in England
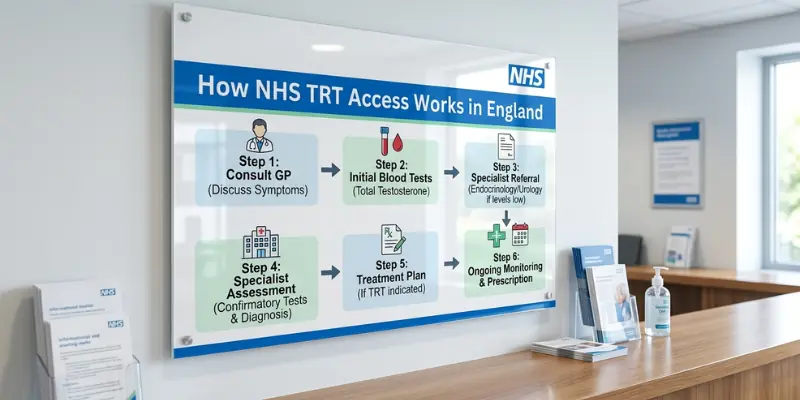
The Clinical Pathway
In the NHS, TRT initiation typically follows a pathway: GP identifies low testosterone on blood test → referral to endocrinology or urology → specialist confirms diagnosis → specialist initiates TRT → GP assumes ongoing prescribing under shared care agreement. In practice, this pathway is frequently blocked, delayed, or circumvented at multiple points.
NICE Guidance and ICB Commissioning

NICE (National Institute for Health and Care Excellence) does not currently have a specific technology appraisal on TRT but recognises hypogonadism as a treatable condition. However, local clinical commissioning decisions — now made by ICBs (Integrated Care Boards), previously by CCGs — determine what is actually funded in each area. In many ICBs, TRT is categorised as a restricted or low-priority treatment, meaning it requires pre-authorisation, specific clinical criteria to be met, or is only funded for certain indications.
In Yorkshire, the relevant ICBs — NHS West Yorkshire ICB, NHS Humber and North Yorkshire ICB — each have their own commissioning policies. These policies frequently stipulate that TRT is funded only for men with clearly pathological hypogonadism (such as Klinefelter syndrome, pituitary tumour, or post-surgical gonadal failure) rather than late-onset or lifestyle-related secondary hypogonadism. Men with late-onset hypogonadism — by far the most common presentation in clinical practice — frequently fall outside funded criteria even when they are clinically appropriate candidates for treatment.
The GP Gatekeeping Problem

Even where NHS TRT is theoretically accessible, the GP appointment is the bottleneck for most men. Several issues compound here: many GPs are not familiar with the nuances of testosterone assessment (the importance of morning fasting samples, free testosterone calculation, LH and FSH interpretation); many apply outdated or overly conservative testosterone thresholds; and many are reluctant to refer to endocrinology for symptoms that are attributed — sometimes dismissively — to age, lifestyle, or stress.
The result: men with genuine clinical need frequently do not receive an NHS referral, and those who do face waiting times for specialist appointments that, in some Yorkshire NHS trusts, extend to 12–18 months.
What Private TRT Offers That NHS Typically Cannot
Parameter | NHS TRT Pathway | Private TRT at Vitalis Luxe Clinic |
|---|---|---|
Access | GP referral required; frequently declined for late-onset hypogonadism; dependent on ICB commissioning policy | Direct access — no GP referral needed; assessment on clinical merit, not commissioning criteria |
Wait for initial assessment | 3–18 months for specialist endocrinology via NHS in Yorkshire | Typically within days to weeks; urgent slots available |
Diagnostic scope | 3–18 months for specialist endocrinology via the NHS in Yorkshire | Comprehensive panel: total + free testosterone, SHBG, LH, FSH, oestradiol, prolactin, PSA, haematocrit, metabolic markers |
Consultation time | 10–15 minutes GP appointment; specialist appointments 20–30 minutes | Dedicated 45–60 minute initial consultation; full clinical and symptom assessment |
Treatment options | Often total testosterone only; free testosterone and full panel are less consistently assessed | Full range: injectable enanthate/cypionate, Nebido, gels, cream; preparation chosen based on clinical suitability |
Monitoring frequency and detail | Varies; often annual if stable; less comprehensive panel | Regular structured monitoring: 6–8 weeks, 3 months, 6-monthly; full panel each time |
Preparation flexibility | Primarily testosterone gels (NHS formulary); injectable TRT is less consistently available; Nebido most common injectable | Clinician-led preparation choice and dose optimisation based on individual response |
Cost | Free at point of use (if accessible and approved) | Monthly subscription or per-appointment fees; medication costs additional — typically £80–£200/month total |
Continuity | Limited by the NHS formulary and prescribing constraints | Consistent clinician relationship; named prescriber throughout treatment |
Shared care | Can request shared care after initiation — GP prescribes under specialist guidance | Shared care letter available for GPs willing to co-prescribe; reduces private prescription costs |
Why Men Are Declining NHS TRT: The Most Common Reasons
1. Testosterone ‘In the Normal Range’
The most common reason for NHS TRT refusal: the man’s testosterone is above the laboratory lower limit of the reference range — even if it is in the lowest 10% of that range and he is significantly symptomatic. NHS GPs often do not distinguish between ‘within the population reference range’ and ‘adequate for this individual patient.’ A testosterone of 9 nmol/L in a symptomatic 55-year-old may be clinically significant but may not trigger an NHS referral.
2. Late-Onset Hypogonadism Not a Funded Indication
Many Yorkshire ICBs restrict TRT funding to men with pathological, young-onset, or clearly structural hypogonadism. Late-onset hypogonadism — the most prevalent form in clinical practice — is frequently categorised as low-priority or excluded from funding. This is a commissioning decision, not a clinical one: the evidence supports treatment for LOH, but funding policy doesn’t always follow the evidence.
3. Single or Poorly Timed Blood Test
NHS guidelines recommend two separate morning fasting testosterone measurements before diagnosing a deficiency. In practice, many GPs test once — often in the afternoon, unfasted — and either dismiss the result as normal or make a clinical decision based on an unreliable single sample. This both understates true deficiency (afternoon tests run 20–35% lower than morning) and fails to meet the diagnostic standard required for treatment initiation.
4. Concerns About Safety That Are Not Supported by Current Evidence
Some GPs decline TRT referral, citing cardiovascular risk, prostate cancer risk, or other safety concerns that are not supported by current evidence in the way they are applied. As discussed in our blogs on cardiovascular safety and prostate health, the evidence base for appropriately prescribed TRT with proper monitoring does not support the level of risk attributed to it in some NHS prescribing decisions.
5. Lack of Familiarity with TRT Monitoring
GPs who are unfamiliar with TRT monitoring requirements — haematocrit, PSA, oestradiol, testosterone levels, and how to interpret and manage changes in each — are understandably reluctant to initiate or continue treatment they don’t feel equipped to manage. This is a capacity and training issue in primary care, not a safety issue with TRT itself, but it produces the same outcome for the patient.
Shared Care: Bridging the NHS–Private Gap
A shared care agreement is a formal arrangement under which a specialist (in this case, a private TRT clinician) initiates treatment and provides a structured protocol, and the patient’s NHS GP takes on ongoing prescribing under that protocol. This arrangement — where the GP is willing — allows patients to access the specialist assessment and initiation that private clinics provide while reducing ongoing private prescription costs by having NHS prescriptions issued by the GP.
In practice, shared care works well where GPs are willing to engage with it. Some Yorkshire GPs are experienced with TRT shared care and agree readily; others are reluctant or decline entirely, citing discomfort prescribing a treatment they did not initiate or unfamiliarity with monitoring requirements. Vitalis Luxe Clinic provides detailed shared care letters — setting out the clinical rationale, monitoring protocol, and contact details — for GPs who are willing to co-prescribe.
Important: GPs are not obligated to accept shared care arrangements. If your GP declines, private prescription continues. The Vitalis Luxe Clinic team can advise on the shared care conversation with your GP and provide the clinical documentation to support it.
What Private TRT Costs in Yorkshire
Costs for private TRT vary between providers. At Vitalis Luxe Clinic in Hull, the cost structure is transparent and designed to be sustainable for long-term treatment:
- Initial consultation — comprehensive assessment including clinical history, hormone panel interpretation, PSA, and treatment planning
- Blood tests — either home kit or clinic phlebotomy; initial panel and regular monitoring tests
- Medication — private prescription for testosterone preparation; cost varies by preparation (injectable typically most cost-effective)
- Monitoring appointments — structured review appointments at 6–8 weeks, 3 months, and 6-monthly
The total monthly cost of private TRT — consultation, monitoring, and medication combined — typically ranges from £80 to £200 per month depending on preparation choice, monitoring frequency, and consultation structure. Injectable testosterone enanthate is generally the most cost-effective preparation on private prescription. Testosterone gels, while convenient, tend to be more expensive on private prescription due to their higher cost per dose.
For men who achieve shared care with their GP, NHS prescription of the testosterone preparation reduces ongoing costs substantially, to the cost of monitoring appointments and any private prescriptions for preparation not available on the NHS formulary.
Practical Steps for Men Seeking TRT in Yorkshire
If You Want to Try the NHS First
- Request a morning fasting testosterone test from your GP — specify that you want it first thing in the morning, fasted
- Ask for LH and FSH to be included alongside testosterone — this distinguishes primary from secondary hypogonadism and strengthens the referral case
- If declined, ask your GP to document the reason in writing — this is useful if you pursue the decision through the practice manager or ICB
- If referred, ask about waiting times — in many Yorkshire NHS trusts, endocrinology waits are 12+ months; this is relevant to your decision about private alternatives
- If your GP is unfamiliar with TRT or dismissive of your symptoms, you have the right to request a second opinion or a referral to a GP with a special interest in men’s health or endocrinology
If You Are Considering Going Private
- Verify that the clinic uses a registered clinician — GP, nurse prescriber, or specialist — not unlicensed practitioners
- Confirm that PSA is assessed before any prescribing begins — non-negotiable
- Check the monitoring protocol — haematocrit, testosterone, oestradiol, and PSA should all be part of regular monitoring
- Ask about shared care — whether the clinic provides shared care letters and whether your GP is likely to accept co-prescribing
- Ask about the full cost, including monitoring and blood tests — not just the consultation fee
Frequently Asked Questions
Can I get TRT on the NHS in Yorkshire?
TRT is available on the NHS in Yorkshire, but access is significantly restricted. Most Yorkshire ICBs fund TRT primarily for men with clearly pathological, young-onset, or structural hypogonadism — Klinefelter syndrome, pituitary tumours, post-surgical failure. Men with late-onset hypogonadism — the most common presentation — frequently fall outside funded criteria even when they are clinically appropriate candidates. NHS waiting times for specialist endocrinology review can extend to 12–18 months in some Yorkshire trusts.
My GP says my testosterone is normal — can I still get TRT privately?
Yes — private TRT clinics assess clinical suitability on the basis of symptoms, free testosterone (not just total testosterone), LH and FSH, and the full clinical picture rather than NHS commissioning criteria. A testosterone result that falls within the wide laboratory reference range may still represent a clinically significant deficiency for an individual patient, particularly if free testosterone is low, symptoms are significant, and other causes have been excluded. At Vitalis Luxe Clinic, we provide a comprehensive assessment that makes this clinical determination.
How long does it take to start TRT through a private clinic in Hull?
At Vitalis Luxe Clinic, the pathway from initial enquiry to treatment initiation is typically a matter of weeks rather than months. Initial consultation, blood tests, result review, and treatment planning can usually be completed within 2–4 weeks, depending on test turnaround and clinical complexity. This compares to 12–18 months for NHS endocrinology referral in many Yorkshire trusts.
Will my GP prescribe TRT if I get it started privately?
Some GPs in Yorkshire will accept a shared care arrangement and prescribe testosterone on NHS prescription once a private specialist has initiated treatment and provided a detailed shared care letter. Others decline, citing discomfort with prescribing a treatment they didn’t initiate or unfamiliarity with monitoring requirements. Vitalis Luxe Clinic can provide shared care letters and clinical documentation to support the request. If your GP declines, private prescription continues — typically, the most cost-effective private preparation is injectable testosterone enanthate.
Is private TRT as safe as NHS TRT?
The clinical safety of TRT depends on the pre-treatment assessment and ongoing monitoring — not on whether it is prescribed privately or on the NHS. A private TRT clinic that performs comprehensive pre-treatment assessment (PSA, haematocrit, testosterone panel, cardiovascular history) and maintains structured regular monitoring is clinically safer than an NHS pathway that prescribes without adequate baseline or fails to monitor appropriately. Vitalis Luxe Clinic’s monitoring protocol is built on the BSSM guidelines and the same clinical standards that govern NHS endocrinology practice.
Can I get TRT without seeing a doctor in person?
Online TRT services with home blood testing allow assessment and initiation without in-person consultation. This is clinically appropriate when the online assessment is conducted by a registered prescriber, includes a comprehensive blood panel (including PSA), involves a proper clinical consultation, and is followed by structured monitoring. The absence of in-person assessment does not preclude safe prescribing if these elements are present. Vitalis Luxe Clinic offers both in-person and remote assessment options for men across Yorkshire.
What happens if I stop paying for private TRT — will I lose my medication?
If you stop your private subscription, your private prescription will not be renewed. However, if you have achieved shared care with your NHS GP, they may continue prescribing on the NHS. Alternatively, you can request a referral from your private clinic back to your GP for NHS consideration — often with improved prospects now that you have documented evidence of both diagnosis and positive treatment response. Treatment continuity is an important consideration to discuss with your private prescriber from the outset.
Why choose Vitalis Luxe Clinic in Hull over an online-only TRT service?
Vitalis Luxe Clinic offers the combination of in-person clinical assessment at our Hull clinic — including examination where indicated, face-to-face consultation, and the ability to manage complications in person — alongside the flexibility of remote monitoring with home blood testing for men across Yorkshire. We provide both the accessibility of online services and the clinical depth of in-person care. We serve men across Hull, East Yorkshire, and throughout Yorkshire.