






At Vitalis Luxe Clinic in Hull, our position is grounded in the physiology: oestradiol is not an unwanted side effect of TRT — it is a biologically necessary hormone in men, and its management requires nuance rather than reflexive suppression. This article explains the full picture.
Oestradiol is the most misunderstood hormone in TRT management. Online forums are filled with men aggressively suppressing their oestradiol with aromatase inhibitors — often causing more harm than the elevated TRT oestradiol VitalisLuxe they were trying to avoid. Clinics are divided between those who routinely add anastrozole to every TRT protocol and those who use aromatase inhibitors rarely, if at all. Men are confused about what oestradiol is, what it does, when elevated levels are problematic, and what to do about it.
Table of Contents
Why Men Have Oestradiol and Why It Matters
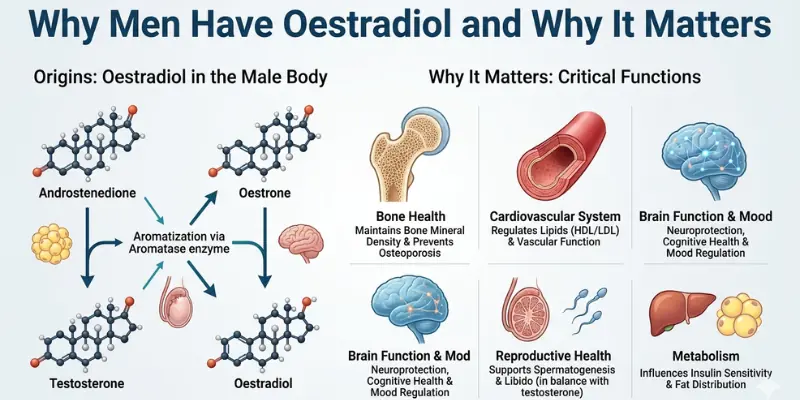
Testosterone is converted to oestradiol (the primary oestrogen in both men and women) by the enzyme aromatase, present in adipose tissue, muscle, brain, liver, and bone. In men, circulating oestradiol comes almost entirely from peripheral aromatisation of testosterone — a small fraction is also produced directly by the testes.
Oestradiol in men serves essential physiological functions that are frequently overlooked in the Testosterone Replacement Therapy community’s preoccupation with testosterone:
- Bone health — oestradiol is the dominant bone-protective hormone in men; more important than testosterone itself for bone mineral density maintenance; men with aromatase deficiency or oestrogen receptor mutations develop severe osteoporosis despite normal testosterone
- Cardiovascular protection — oestradiol has vasodilatory effects and supports endothelial function; very low oestradiol on TRT is associated with adverse lipid profiles and increased cardiovascular risk
- Libido and sexual function — counterintuitively, oestradiol contributes to sexual desire and erectile function in men; too-low oestradiol from aggressive AI use can significantly impair libido
- Cognitive function — oestradiol has neuroprotective effects; deficiency is associated with cognitive decline
- Joint health — men with very low oestradiol commonly report joint pain and reduced flexibility
- Mood — oestradiol contributes to serotonergic tone; excessively low levels are associated with anxiety, irritability, and low mood — the same symptoms attributed to high oestradiol
The clinical implication: oestradiol deficiency from over-aggressive AI use produces a syndrome virtually identical to the high-oestradiol syndrome men are trying to avoid — and adds bone loss and cardiovascular risk that high oestradiol alone does not cause.
The Normal Range for Oestradiol in Men on TRT
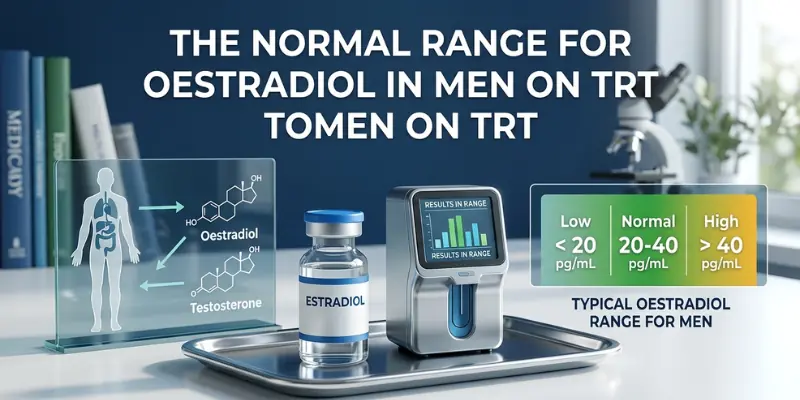
UK laboratory reference ranges for oestradiol in men vary, but most report the normal male range as approximately 40–190 pmol/L (approximately 11–52 pg/mL in US units). On TRT, oestradiol rises as testosterone rises — this is expected and physiological. Most TRT clinicians target oestradiol in the upper-normal to mildly above-normal range — typically 100–200 pmol/L — rather than at the lower end of the reference range, because the physiological benefits of oestradiol are dose-dependent within the normal range.
Oestradiol Level | Clinical Interpretation | Typical Action |
|---|---|---|
Below 70 pmol/L on TRT | Low — potential deficiency state; common after over-aggressive AI use | Reduce or stop AI; adjust TRT preparation if applicable |
70–150 pmol/L | Normal-low to normal — acceptable; may be appropriate target for some men | Monitor; assess for symptoms; no AI typically needed |
150–250 pmol/L | Normal-high — within or slightly above reference range on TRT | Monitor; assess for symptoms; no AI needed unless symptomatic |
250–350 pmol/L | Mildly elevated on TRT — common in overweight or higher-dose protocols | Assess symptoms specifically; AI only if symptomatic with attributable symptoms |
Above 350 pmol/L | Significantly elevated | Lifestyle intervention (weight loss); TRT dose review; AI if symptomatic and confirmed elevated |
Symptoms of High Oestradiol vs. Low Oestradiol on TRT
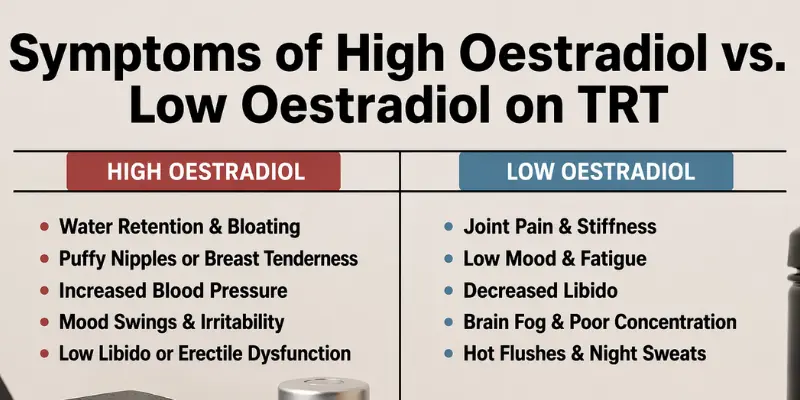
The inability to distinguish high from low oestradiol symptoms without a blood test is one of the most clinically important points in TRT management. The two conditions overlap substantially:
Symptom | High Oestradiol | Low Oestradiol (AI Over-Suppression) |
|---|---|---|
Gynaecomastia (breast tissue growth) | Present — the most specific high-E2 symptom | Absent — does not occur with low E2 |
Mood changes/irritability | Common | Uncommon |
Nipple sensitivity/tenderness | Common | Absent |
Mood changes / irritability | Present | Present — very similar presentation |
Reduced libido | Present — paradoxical | Present — very common; often the main complaint |
Erectile dysfunction | Present | Present — often worse than with high E2 |
Fatigue | Present | Present |
Joint pain | Uncommon | Very common — a hallmark of low E2 |
Bone symptoms | Uncommon in short term | Increased fracture risk with sustained low E2 |
Cardiovascular lipid effects | Variable | Adverse — reduced HDL, increased LDL tendency |
When Aromatase Inhibitors Are and Are Not Appropriate
When AI May Be Appropriate
- Confirmed elevated oestradiol (>300–350 pmol/L on a well-timed sample) with specific attributable symptoms — particularly gynaecomastia, significant water retention, or confirmed nipple tenderness
- Men with significant obesity where aromatase activity is high and oestradiol elevation is persistent despite dose and lifestyle management
- Men in whom oestradiol elevation is causing confirmed HPG axis suppression effects (in clomifene protocols)
When AI Is Not Appropriate
- Oestradiol in the normal or mildly elevated range without specific symptoms — routine prophylactic AI use is not supported by clinical evidence and risks iatrogenic deficiency
- Symptoms attributable to high oestradiol without a confirming blood test — symptoms must be matched to confirmed biochemical elevation
- Joint pain, low mood, or reduced libido attributed to high oestradiol without testing — these symptoms are more consistent with low oestradiol than high
- Men with oestradiol already in the lower portion of the normal range who are experiencing symptoms — AI will worsen the situation
AI Options
The two most commonly used AIs in TRT management are anastrozole (non-steroidal, reversible; typically 0.25–0.5mg twice weekly) and exemestane (steroidal, irreversible; typically 12.5–25mg twice weekly). Anastrozole is more commonly used; exemestane is preferred by some clinicians for its steroidal structure and different side effect profile. Both require oestradiol monitoring to avoid over-suppression.
Managing Oestradiol Without an AI
Before reaching for an aromatase inhibitor, several approaches can reduce oestradiol naturally:
- Visceral fat reduction — aromatase is concentrated in adipose tissue; meaningful weight loss reduces aromatase activity and oestradiol conversion substantially
- Injection frequency — twice-weekly injections of testosterone enanthate produce lower peak-trough testosterone fluctuation than weekly injections, reducing the oestradiol peaks associated with high testosterone spikes
- Preparation switch — from scrotal cream (very high DHT and oestradiol conversion through skin aromatase) to injectable, which produces lower and more stable oestradiol
- Dose optimisation — if testosterone is running supraphysiological, dose reduction reduces aromatisation proportionally
Frequently Asked Questions
What is oestradiol and why do men have it on TRT?
Oestradiol is the primary oestrogen in both men and women. In men, it is produced primarily by the conversion of testosterone to oestradiol by the enzyme aromatase, which is present in fat tissue, muscle, liver, and brain. When TRT raises testosterone, oestradiol rises proportionally. This is physiologically normal and expected — oestradiol serves essential functions in men including bone protection, cardiovascular health, joint health, cognitive function, and sexual function. The goal is oestradiol balance, not oestradiol suppression.
What are the symptoms of high oestradiol on TRT?
The most specific symptoms of genuinely high oestradiol are gynaecomastia (breast tissue growth or enlargement), nipple tenderness, and significant water retention. Mood changes, reduced libido, and fatigue also occur but are non-specific — they overlap closely with symptoms of low oestradiol from over-suppression. Oestradiol must be confirmed by blood test before symptoms are attributed to high levels and an aromatase inhibitor considered.
Do I need an aromatase inhibitor on TRT?
Most men on TRT do not need an aromatase inhibitor. AI use is appropriate only when oestradiol is confirmed elevated by blood test and specific attributable symptoms are present — particularly gynaecomastia or significant water retention. Routine prophylactic AI use to keep oestradiol at the lower end of the normal range is not clinically supported and risks iatrogenic oestradiol deficiency, which causes joint pain, reduced libido, adverse lipid effects, and bone loss. At Vitalis Luxe Clinic, AI use is selective and always guided by oestradiol blood testing.
What happens if oestradiol is too low on TRT?
Low oestradiol on TRT — most commonly caused by aggressive AI use or high-DHT preparations in men with lower body fat — produces a characteristic syndrome: joint pain (often the most prominent symptom), reduced libido and erectile dysfunction, mood changes including anxiety and irritability, fatigue, and adverse lipid profile changes. Sustained low oestradiol also causes bone loss, as oestradiol is the dominant bone-protective hormone in men. Treatment is the reduction or cessation of AI and oestradiol recheck.
What should my oestradiol be on TRT?
Most UK TRT clinicians target oestradiol in the upper half of the normal male reference range — approximately 100–200 pmol/L — on TRT, rather than at the lower end. Oestradiol in this range supports bone health, cardiovascular protection, joint health, and libido without producing the specific high-oestradiol symptoms of gynaecomastia and water retention. Oestradiol above 300–350 pmol/L with symptoms may warrant intervention; oestradiol below 70–80 pmol/L is deficient and associated with significant side effects.
Can I manage high oestradiol without an aromatase inhibitor?
Yes — the primary approaches to oestradiol management without AI are: visceral fat reduction (reduces aromatase activity substantially); injection frequency optimisation (twice-weekly reduces testosterone peaks and oestradiol spikes versus once-weekly); preparation switch if applicable (injectable rather than scrotal cream); and dose optimisation if testosterone is supraphysiological. These approaches are preferable to AI where possible because they address the underlying cause rather than pharmacologically suppressing a hormone with important physiological functions.
Where can I get oestradiol managed properly on TRT in Hull or Yorkshire?
Vitalis Luxe Clinic includes oestradiol as part of every monitoring blood panel — at 6–8 weeks, 3 months, and 6-monthly throughout TRT. AI decisions are made on the basis of confirmed blood test results and specific symptom assessment, not symptom attribution alone. We serve men across Hull, East Yorkshire, and throughout Yorkshire — in person or online with home blood testing.