





If you spend any time in men’s health forums, NoFap communities, or fitness-focused corners of the internet, you will have encountered the claim that edging — the practice of prolonging sexual arousal while delaying or avoiding orgasm — dramatically increases testosterone levels. The theory is presented with considerable confidence: abstinence from ejaculation raises T, edging harnesses sexual energy without losing it, and the result is elevated testosterone with all its associated benefits.
It’s a compelling idea. It’s also largely unsupported by the clinical evidence.
At Vitalis Luxe Clinic we take a measured, evidence-based approach to every claim about testosterone — whether it comes from a clinical trial or an online forum. In this article, we’ll look honestly at what the research actually says about edging, ejaculation frequency, abstinence, and Testosterone Replacement Therapy levels. We’ll explain the physiological reality, address the specific studies that are typically cited in these communities, and help you understand what actually has a meaningful impact on your testosterone — so you can focus your energy where it genuinely matters.
We’ll also address this topic with the clinical directness it deserves — without embarrassment, and without moralizing. Sexual health is a core component of men’s overall well-being, and it deserves the same evidence-based treatment as any other aspect of health.
Table of Contents
What Is Edging and Why Do Men Think It Raises Testosterone?
Edging refers to the practice of repeatedly bringing oneself (or a partner) close to the point of orgasm and then pulling back — extending the arousal phase while delaying or avoiding ejaculation entirely. It is practised both as a sexual technique for prolonging pleasure and, increasingly, as part of broader “semen retention” or NoFap protocols in online communities that attribute significant health and hormonal benefits to ejaculation avoidance.
The testosterone connection is typically argued along the following lines: testosterone is somehow “used up” or “lost” through ejaculation; therefore, retaining semen preserves testosterone. Edging, the argument goes, allows the physiological arousal associated with sexual stimulation — which proponents claim raises testosterone — without the supposed testosterone loss of ejaculation.
Neither premise of this argument is supported by the clinical evidence. Ejaculation does not meaningfully deplete testosterone. And while sexual arousal produces a modest, transient hormonal response, the sustained testosterone-raising effect of edging is not demonstrated in controlled research.
To understand why, we need to look at what the evidence actually shows about the relationship between sexual behaviour and testosterone levels.
What Does the Research Actually Say?
The Most Cited Study: The 7-Day Abstinence Peak
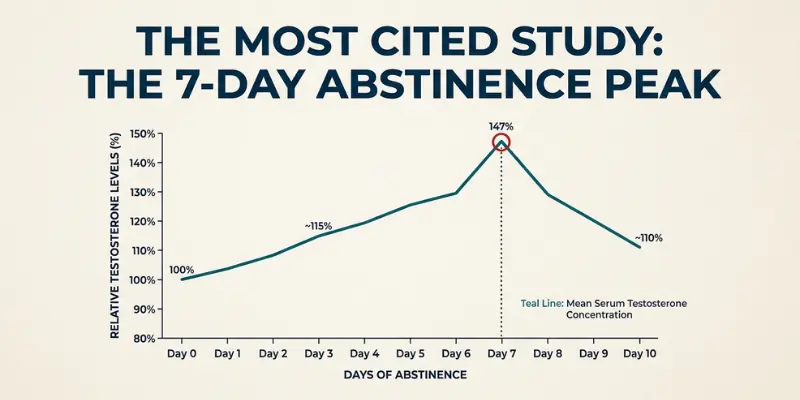
The study most frequently referenced in support of edging and semen retention claims is a 2003 Chinese study by Jiang et al., which examined serum testosterone levels in 28 men over a period of sexual abstinence. The study found that testosterone levels remained relatively stable for the first six days of abstinence, peaked sharply on day seven — reaching approximately 145% of baseline — and then returned toward baseline levels thereafter.
This finding is real, replicated in the sense that abstinence-related testosterone fluctuations have been observed by other researchers, and is the legitimate scientific kernel at the centre of much of the semen retention discussion. But it is widely misrepresented in online communities, and it is worth unpacking exactly what it means — and what it doesn’t.
What the Jiang Study Actually Tells Us
- The testosterone peak on day seven was transient — levels returned toward baseline after the peak, not continuing to rise with extended abstinence
- The study was small (28 men) and did not include long-term follow-up — we do not know what happens to testosterone levels over weeks or months of sustained abstinence
- The peak, while statistically significant, was a temporary fluctuation within the physiological range — not a clinically meaningful, sustained elevation that would translate into the effects men associate with high testosterone
- Crucially, the study measured abstinence from ejaculation, not edging specifically — the two are not equivalent, and edging was not studied
In other words, the study shows a temporary spike in testosterone around day seven of abstinence, followed by a return toward baseline. It does not show that continued abstinence produces sustained high testosterone, and it tells us nothing specific about edging.
Other Studies on Sexual Behaviour and Testosterone
The broader research on ejaculation frequency and testosterone is inconsistent and does not support the idea that abstinence or restricted ejaculation meaningfully raises baseline testosterone in healthy men:
- Some studies in healthy men have found no significant difference in resting testosterone between men with high versus low ejaculation frequency
- Studies examining masturbation and testosterone have generally found only transient, modest acute changes that return to baseline within hours
- Research on men in committed relationships has found that testosterone is influenced more by relationship status, sexual behaviour within relationships, and social context than by ejaculation frequency per se
- Animal studies — which are sometimes cited in online discussions — involve species with very different reproductive physiology and should not be extrapolated to human hormonal response
The Physiology: Why Ejaculation Doesn’t Deplete Testosterone
The core premise of semen retention — that ejaculation depletes testosterone — is physiologically unfounded. Understanding why helps clarify why the entire framework is built on a misconception.
Testosterone is produced by Leydig cells in the testes in response to luteinizing hormone (LH) from the pituitary gland. This production process is continuous, regulated by the HPG axis feedback loop, and entirely independent of ejaculation frequency. Ejaculation is a muscular and neurological event — it involves the release of seminal fluid from the seminal vesicles and prostate, not the loss of circulating testosterone.
Semen does contain trace amounts of testosterone — but these amounts are clinically negligible relative to the body’s total testosterone production. A man produces 3–10 milligrams of testosterone per day through Leydig cell synthesis. The testosterone content of a typical ejaculate is measured in micrograms — orders of magnitude smaller. The idea that ejaculation meaningfully depletes circulating testosterone is physiologically equivalent to worrying that breathing depletes your oxygen stores.
Sexual arousal and orgasm do produce transient hormonal responses — modest, short-lived increases in prolactin, oxytocin, and other neuroendocrine markers. But these are acute fluctuations that return to baseline within minutes to hours and do not represent meaningful changes in the body’s hormonal setpoint.
Edging Specifically: Is There Any Evidence of Benefit?
Edging has not been specifically studied in relation to testosterone levels in any rigorous clinical research we are aware of. The claims about edging and testosterone are entirely extrapolated from the abstinence literature — specifically, the day-seven testosterone peak in the Jiang study — combined with the reasoning that maintaining arousal without ejaculation would somehow produce a sustained hormonal benefit.
This extrapolation is not supported by evidence. The day-seven peak in the Jiang study occurred in abstinent men, not in men who were regularly aroused without ejaculating. There is no research demonstrating that the hormonal response to edging is different from the hormonal response to masturbation with ejaculation, or that sustained arousal without ejaculation produces meaningfully elevated testosterone over time.
Possible Psychological Effects vs. Hormonal Effects
It is worth distinguishing between the hormonal claims and the psychological and behavioural claims sometimes made about edging and semen retention. Some men in these communities report increased motivation, focus, confidence, and drive during periods of abstinence or reduced ejaculation frequency.
These reported experiences are real — but they may have more to do with behavioural changes associated with the practice (increased discipline, reduced time spent on pornography and related behaviours, improved sleep, reduced anxiety about sexual performance) than with any direct hormonal mechanism. The fact that men feel better does not confirm that testosterone is higher; correlation between a practice and subjective well-being is not evidence of a specific hormonal mechanism.
What Actually Has a Meaningful Impact on Testosterone?

If the online discourse around edging and semen retention reflects a genuine desire to optimize testosterone through lifestyle — which we believe it does for many men — then it deserves an honest answer about where to direct that effort.
The following interventions have substantially stronger evidence for meaningful testosterone support than edging, abstinence, or semen retention:
| Intervention | Evidence Level | Typical Effect on Testosterone |
|---|---|---|
| Heavy compound resistance training | Very strong | Major production occurs during deep sleep; restriction causes a measurable decline |
| Reducing excess visceral body fat | Very strong | Reduces aromatase conversion; can meaningfully raise T over months |
| Optimising sleep (7–9 hours) | Very strong | Zinc is essential for Leydig cell function; deficiency clearly suppresses T |
| Correcting vitamin D deficiency | Moderate | Restoring deficient levels associated with improved T in multiple studies |
| Correcting zinc deficiency | Moderate | Cortisol directly suppresses T at the hypothalamic and testicular level |
| Chronic stress reduction | Moderate | Weak/transient |
| Reducing heavy alcohol consumption | Moderate | Chronic use impairs Leydig cell function and HPG axis signalling |
| 7-day ejaculatory abstinence | Edging/semen retention | Temporary day-7 peak only; returns to baseline; not clinically meaningful |
| Edging/semen retention | No direct evidence | Not studied; claims extrapolated from abstinence data without support |
The contrast is clear. If you want to meaningfully raise your testosterone through lifestyle, your time and energy are far better invested in sleep, resistance training, body composition, and nutritional status than in sexual behaviour modification.
When Interest in Edging Reflects a Deeper Concern
At Vitalis Luxe Clinic in Hull, we have observed a pattern worth acknowledging: men who are actively researching edging, NoFap, and semen retention are often men who are experiencing genuinely low energy, reduced motivation, low libido, and a sense of not being at their best — and they are attempting to address those concerns through lifestyle and behavioural modification.
That impulse is entirely understandable. The concern is real. But in many cases, the underlying cause of what they’re experiencing is not an ejaculation frequency issue — it is clinically low testosterone that no amount of sexual behaviour modification will address.
If you are a man experiencing persistent fatigue, low motivation, significantly reduced libido, difficulty building muscle, brain fog, and low mood — and you have been attempting to address these through semen retention, NoFap, edging, or other behavioural approaches without meaningful improvement — there is a reasonable possibility that your testosterone is clinically low.
The only way to know is a blood test. Not an online calculator. Not a symptom checklist. A morning testosterone blood test, ideally with a full hormone panel including free testosterone, SHBG, LH, FSH, and prolactin, interpreted by a qualified clinician.
At Vitalis Luxe Clinic, we see men from across Hull, East Yorkshire, and throughout Yorkshire who have spent months or years trying to optimize their way out of symptoms that were always going to require clinical treatment. Getting the blood test is invariably the turning point — because it moves the conversation from speculation to evidence, and from lifestyle advice to clinical solutions where clinical solutions are needed.
Sexual Health, Libido, and Testosterone Replacement Therapy
For men who are on TRT or considering it, it is worth addressing the relationship between testosterone replacement therapy and sexual health directly.
Low libido and sexual dysfunction are among the most common and most distressing symptoms of testosterone deficiency — and among the earliest to improve with properly managed TRT. Men on clinically appropriate TRT protocols typically report significant improvements in sexual desire, erectile function, and overall sexual satisfaction as testosterone levels are restored to within the physiological range.
TRT does not create abnormal or compulsive sexual behaviour. It restores the normal hormonal environment that supports healthy sexual function. For many men, the restoration of libido after years of deficiency is one of the most meaningful quality-of-life improvements they experience — alongside the return of energy, mood, and motivation.
Sexual function is also an important monitoring marker during TRT. If libido remains persistently low despite adequate testosterone levels on treatment, this may suggest suboptimal free testosterone, elevated oestradiol, or a psychological component that warrants further assessment. At our Hull clinic, sexual health is an integral part of how we monitor treatment response — not a side issue.
Frequently Asked Questions
Does edging increase testosterone?
There is no clinical evidence that edging specifically increases testosterone levels. The claims about edging and testosterone are extrapolated from a small study showing a transient testosterone peak on day seven of ejaculatory abstinence, which is not the same as edging, and which produced only a temporary fluctuation that returned to baseline. No research has demonstrated that sustained arousal without ejaculation produces meaningful, lasting testosterone elevation.
Does semen retention increase testosterone?
The evidence is very limited. One small study found a transient testosterone peak around day seven of abstinence, after which levels returned toward baseline. No research shows that prolonged semen retention produces sustained, clinically meaningful increases in baseline testosterone. The fundamental premise — that ejaculation depletes testosterone — is not physiologically supported.
Does ejaculation lower testosterone?
No, not in any clinically meaningful way. Testosterone is produced continuously by Leydig cells in the testes and is not meaningfully depleted by ejaculation. Semen contains only trace amounts of testosterone — negligible relative to the body’s daily production of 3–10 milligrams. Ejaculation frequency does not meaningfully affect baseline testosterone levels in healthy men based on current evidence.
What is NoFap, and does it raise testosterone?
NoFap is a behavioural movement encouraging abstinence from pornography and masturbation, often citing testosterone and other health benefits. The limited evidence for direct testosterone effects from NoFap practices reflects the broader abstinence research — a transient day-seven peak, not sustained elevation. Any benefits reported by men practising NoFap are more likely related to behavioural changes (reduced pornography use, improved sleep, more goal-directed activity) than to direct hormonal mechanisms.
What is the best natural way to increase testosterone?
The most evidence-based natural approaches are: consistent compound resistance training (squats, deadlifts, bench press), achieving and maintaining a healthy body composition (particularly reducing excess visceral fat), prioritizing seven to nine hours of quality sleep per night, correcting any nutritional deficiencies (vitamin D, zinc, magnesium), managing chronic stress and cortisol levels, and reducing heavy alcohol consumption. These interventions produce substantially greater and more sustained testosterone support than any sexual behaviour modification.
Could my low energy and libido be low testosterone rather than something I can fix through lifestyle?
Possibly — and this is exactly the question a blood test is designed to answer. If you have been experiencing persistent fatigue, reduced libido, low motivation, and difficulty maintaining muscle mass, and lifestyle optimisation has not produced meaningful improvement, a comprehensive hormone panel at Vitalis Luxe Clinic in Hull will clarify whether clinically low testosterone is the underlying cause.
Does testosterone affect sexual desire?
Yes, significantly. Testosterone is the primary hormonal driver of libido in men. Clinically low testosterone is associated with substantially reduced or absent sexual desire, reduced morning erections, and impaired erectile function. Restoring testosterone to within the physiological range through properly managed TRT is associated with meaningful improvements in libido and sexual function in the majority of men with confirmed deficiency.
Where can I get my testosterone checked in Hull or Yorkshire?
Vitalis Luxe Clinic provides comprehensive testosterone blood testing and clinician-led hormone assessments for men across Hull, East Yorkshire, Beverley, Cottingham, Hessle, Willerby, York, and the wider Yorkshire region. No GP referral is required. Appointments are available in person at our Hull clinic or via our online consultation service with home blood testing.