





When men start testosterone replacement therapy, one of the most commonly overlooked consequences is what happens to the body’s own hormonal signalling — the HPG axis that normally drives the testes to produce testosterone and sperm. Standard TRT suppresses this axis completely, causing the testes to receive no stimulatory signals and, over time, to reduce in size and cease spermatogenesis. For men who have completed their family and are not concerned about fertility, this is an acceptable trade-off. For men who want to preserve fertility, testicular size, or their own residual production, human chorionic gonadotropin (hCG) provides a practical solution.
At Vitalis Luxe Clinic, hCG co-prescription is discussed with every patient for whom it is relevant — particularly younger men, those with fertility considerations, and those who want to maintain the appearance and function of their testes on long-term TRT and hCG Protocol . This article explains how hCG works, what it achieves, how it is used, and when it is the right addition to a TRT protocol.
Table of Contents
The Problem: What Standard TRT Does to the HPG Axis
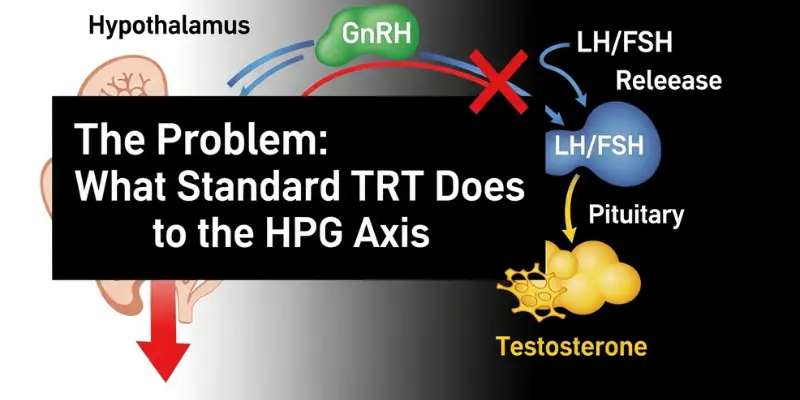
The hypothalamic-pituitary-gonadal (HPG) axis operates on negative feedback: when testosterone levels are adequate, the hypothalamus reduces GnRH pulsing, the pituitary reduces LH and FSH release, and the testes reduce production. When exogenous testosterone is introduced through TRT, circulating testosterone rises — and the HPG axis interprets this as excess. GnRH, LH, and FSH all suppress, often to near-zero, within weeks of starting TRT.
The consequences are predictable: without LH stimulation, the Leydig cells of the testes have no signal to produce testosterone or support spermatogenesis; without FSH, the Sertoli cells that support sperm production become quiescent. The result is testicular atrophy — progressive reduction in testicular volume — and azoospermia — absence of sperm in the ejaculate — in the majority of men within 3–6 months of starting TRT.
For men who have definitively completed their family and are not concerned about testicular size, this is clinically manageable. For others, it is a significant concern — and hCG directly addresses it.
What Is hCG and How Does It Work?
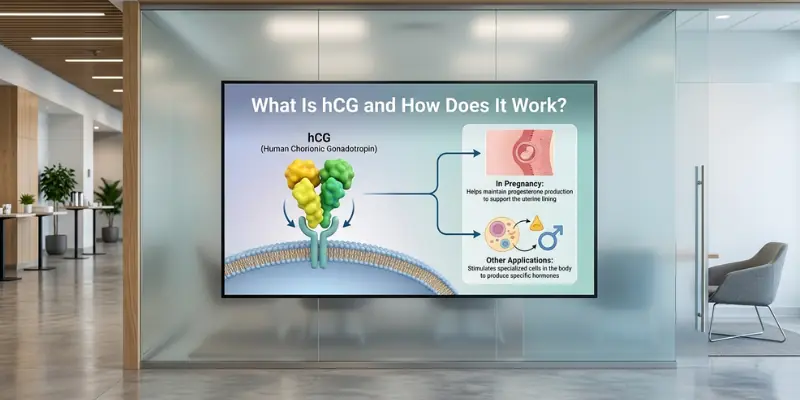
Human chorionic gonadotropin (hCG) is a glycoprotein hormone produced naturally during pregnancy. Its structure closely resembles LH — it shares the same beta subunit binding site as LH at the LH receptor on Leydig cells. This means hCG acts as a functional LH analogue: when injected, it binds to LH receptors on the testes, stimulating Leydig cell testosterone production and — through Leydig cell support of the seminiferous tubules — supporting FSH-independent aspects of spermatogenesis.
Crucially: hCG works directly at the testes, bypassing the suppressed hypothalamus and pituitary entirely. Even while the HPG axis is fully suppressed by exogenous TRT, hCG can maintain Leydig cell stimulation, preserve testicular volume, and support sperm production — because it does not rely on the signalling pathway that TRT has suppressed.
What hCG Achieves on TRT

Outcome | Without hCG on TRT | With hCG Co-Prescribed |
|---|---|---|
Testicular volume | Progressive atrophy — typically 20–40% volume reduction over 6–18 months | Maintained at or near pre-TRT volume in most men |
Spermatogenesis | Near-universal azoospermia within 3–6 months | Partially maintained in many men; significantly better sperm counts than TRT alone |
Intratesticular testosterone | Dramatically reduced — Leydig cells not stimulated | Maintained — Leydig cell stimulation preserved via hCG LH-receptor binding |
Oestradiol levels | May be lower (less testicular oestradiol production) | Typically higher — hCG stimulates testicular oestradiol alongside testosterone; oestradiol monitoring important |
LH and FSH | Both suppressed to near-zero by exogenous TRT | LH suppressed; hCG provides functional LH-like signal; FSH still suppressed (hCG does not mimic FSH) |
Fertility potential | Very low — azoospermia limits fertility severely | Meaningfully better — though not equivalent to pre-TRT; dedicated fertility protocols (hCG + FSH) may be needed for conception attempts |
The hCG Protocol: Dose, Frequency, and Administration
hCG for male HPG axis support is typically prescribed at 500–1,500 IU subcutaneously 2–3 times per week, though protocols vary between clinicians and are individualised based on testicular response and oestradiol levels. The subcutaneous injection is similar in technique to insulin injection — a very fine needle into the fatty tissue of the abdomen or thigh — and most men become comfortable with self-administration within a few sessions.
- Lower doses (500 IU 2–3x/week) maintain testicular function with less oestradiol elevation — appropriate for men prioritising testicular preservation over maximal spermatogenesis
- Higher doses (1,000–1,500 IU 2–3x/week) provide more robust stimulation and are typically used where spermatogenesis is the priority — such as men attempting conception on TRT
- Oestradiol monitoring is essential on hCG — the LH-like stimulation of testicular oestradiol production can push oestradiol levels higher than TRT alone; elevated oestradiol causes gynaecomastia, mood changes, and water retention
- hCG is supplied as a lyophilised (freeze-dried) powder requiring reconstitution with bacteriostatic water; reconstituted vials are stored refrigerated and used over 30 days
Gonadorelin: The Alternative to hCG

Gonadorelin (synthetic GnRH) is increasingly used as an alternative to hCG in TRT protocols. Unlike hCG — which acts directly on the testes — gonadorelin acts at the pituitary, stimulating LH and FSH release. When administered at the right pulsatile frequency (typically via subcutaneous injection every 2–3 days), it can maintain pituitary function and stimulate both LH and FSH — providing a more physiological pattern of testicular stimulation than hCG alone, which only replaces LH.
Gonadorelin is particularly valuable for men who develop excessive oestradiol elevation on hCG — because gonadorelin stimulates endogenous LH at lower effective doses, the oestradiol-driving effect can be lower. It is also the preferred agent for men who want to maintain FSH-driven spermatogenesis more completely. Availability and cost vary; at Vitalis Luxe Clinic, both hCG and gonadorelin options are discussed with eligible patients.
Who Should Consider hCG Alongside TRT?
- Men who have not yet completed their family and want to preserve at least some fertility potential while on TRT
- Men who are concerned about testicular atrophy for psychological or physical reasons
- Men who want to maintain their intratesticular testosterone environment — which may support libido and sexual function beyond what exogenous TRT alone provides
- Men who are considering discontinuing TRT in future and want to maintain testicular responsiveness to make recovery easier
- Men using clomifene who want an additional LH-receptor stimulus
Frequently Asked Questions
Does hCG prevent testicular atrophy on TRT?
Yes — hCG co-prescription with TRT reliably prevents the testicular atrophy that occurs from HPG axis suppression. By stimulating LH receptors on Leydig cells directly, hCG maintains the testicular stimulation that exogenous testosterone removes through pituitary suppression. Most men on hCG maintain testicular volume at or near their pre-TRT size.
Can you get someone pregnant while on TRT with hCG?
Fertility on TRT with hCG is meaningfully better than TRT alone, but not equivalent to pre-TRT fertility. hCG maintains some spermatogenesis, but FSH remains suppressed on standard TRT, limiting spermatogenic support. Men actively trying to conceive may need a dedicated fertility protocol — typically hCG plus FSH injections — under specialist guidance, or a temporary switch from TRT to clomifene.
How quickly does testicular atrophy happen on TRT without hCG?
Testicular atrophy begins within weeks of starting TRT as LH suppression reduces Leydig cell stimulation. Measurable volume reduction typically becomes apparent within 2–4 months and progresses over 6–18 months of continued TRT without hCG. The degree varies — some men lose 20–30% of testicular volume; others less. Starting hCG early — ideally at TRT initiation — prevents atrophy from occurring rather than attempting to reverse established volume loss.
Does hCG affect TRT effectiveness?
hCG does not reduce TRT effectiveness. It adds its own stimulation at the testes without interfering with the exogenous testosterone from TRT. The main clinical consideration is oestradiol elevation from hCG-stimulated testicular oestradiol production — which requires monitoring and occasional management with dose adjustment or aromatase inhibition.
What is the difference between hCG and gonadorelin in TRT?
hCG acts directly on testicular LH receptors, stimulating Leydig cells without involving the pituitary. It replaces only the LH signal — FSH remains suppressed. Gonadorelin acts at the pituitary, stimulating both LH and FSH release, providing a more physiological stimulus that supports both Leydig cell function and FSH-driven spermatogenesis. Gonadorelin is preferred where complete HPG axis preservation is the goal; hCG is more widely available, better studied in this application, and appropriate for most men prioritising testicular preservation over maximal sperm production.
Is hCG available in Hull and Yorkshire?
Yes — Vitalis Luxe Clinic in Hull prescribes hCG as part of comprehensive TRT protocols for eligible patients across Hull, East Yorkshire, and throughout Yorkshire. hCG is prescribed on private prescription following assessment confirming it is clinically appropriate. Training in self-administration technique is provided at the clinic.
Can I start hCG after I’ve already been on TRT for a while?
Yes — hCG can be added to an existing TRT protocol at any stage. Men who started TRT without hCG and subsequently want to preserve or attempt to restore testicular function can add hCG. Some degree of testicular recovery typically occurs with hCG even after established atrophy, though full restoration of pre-TRT volume is not always achievable. Earlier addition produces better outcomes.
Where can I get hCG with TRT in Yorkshire?
Vitalis Luxe Clinic in Hull provides hCG co-prescription as part of individualised TRT protocols for men across Hull, East Yorkshire, and throughout Yorkshire. Discuss your fertility goals and testicular function preferences at your initial consultation and we will build a protocol designed to meet your specific priorities.