






There’s a common assumption that low testosterone is something that happens to older men — a gradual, inevitable consequence of ageing that starts to matter in your fifties or sixties. For many men in their twenties, thirties, or early forties who are experiencing the classic symptoms of What Causes Low testosterone in Young Males deficiency, that assumption creates a significant barrier to getting help.
They dismiss what they’re feeling. They assume it must be stress, overwork, or not sleeping enough. They don’t consider that their hormones might actually be clinically low — because, after all, they’re young.
But low testosterone is not exclusively a condition of older men. Research suggests that testosterone levels have been declining in younger male populations over recent decades, and clinical testosterone deficiency in men under 40 is considerably more common than most people — including many GPs — recognise.
At Vitalis Luxe Clinic in Hull, we see men in their twenties and thirties presenting with significant testosterone deficiency regularly. In this article, we’ll explain the specific causes of low testosterone in younger men, the risk factors that make some individuals particularly vulnerable, and what a proper clinical assessment looks like if you’re concerned about your own hormone levels.
Table of Contents
Why Young Men Can Have Low Testosterone

Testosterone levels in men typically peak in the late teens and early twenties, then decline gradually at approximately 1–2% per year from around age 30. This age-related decline is expected. However, there is a significant difference between the gradual, age-associated decline seen in healthy older men and the clinically significant deficiency that can affect men at any age.
Low testosterone in younger men — sometimes referred to as hypogonadism or testosterone deficiency syndrome (TDS) — can arise from two distinct pathways:
- Primary hypogonadism — the testes themselves are unable to produce adequate testosterone despite receiving the correct hormonal signal from the brain. This may be congenital (present from birth), acquired through injury, illness, or treatment, or idiopathic (no identifiable cause).
- Secondary hypogonadism — the testes are capable of producing testosterone but are not receiving adequate stimulation from the pituitary gland (via luteinising hormone, LH). This is more common in younger men and is frequently driven by lifestyle, metabolic, and psychological factors that are, in many cases, modifiable.
Understanding which pathway is driving the deficiency matters clinically — it affects both the investigation process and the treatment approach. This is one of the reasons a comprehensive hormone panel, rather than a single testosterone reading, is essential for proper diagnosis.
Lifestyle Causes of Low Testosterone in Young Men
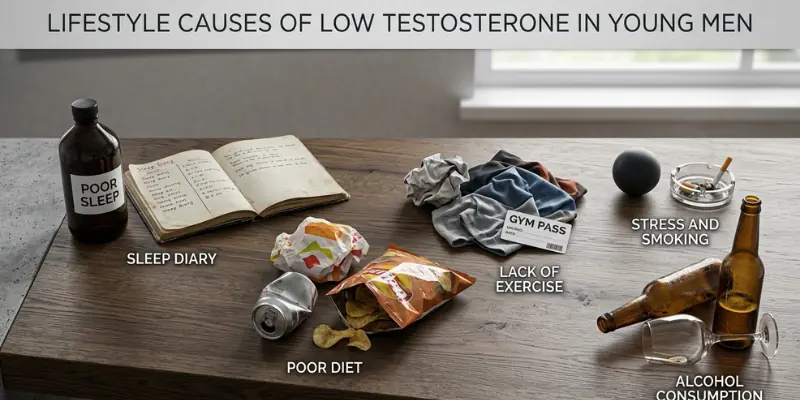
For a significant proportion of younger men with low testosterone, lifestyle factors are the primary drivers — or at least major contributors. These are also, crucially, the most modifiable causes, which is why understanding them is both clinically and practically important.
Obesity and High Body Fat — Particularly Visceral Fat
Excess body fat — and specifically visceral fat, the metabolically active fat stored deep in the abdomen around internal organs — is one of the most significant drivers of testosterone suppression in young men. Visceral fat contains the enzyme aromatase, which converts testosterone into oestrogen. As body fat increases, aromatase activity increases, and circulating testosterone progressively declines.
This creates a damaging feedback loop: lower testosterone makes it harder to build muscle and easier to gain fat, which increases aromatase activity further, driving testosterone even lower. For many younger men, this cycle begins with weight gain in the mid-to-late twenties and accelerates through the thirties if not addressed.
Population studies have consistently found that obesity is strongly correlated with hypogonadism — in some research, obese men have testosterone levels equivalent to those of men 10–15 years their senior.
Chronic Psychological and Physiological Stress
Modern working life — particularly for men in their twenties and thirties managing demanding careers, financial pressures, and family responsibilities — is a significant source of chronic stress. And chronic stress has a direct, measurable, suppressive effect on testosterone production.
The mechanism is well understood: the body produces cortisol (the primary stress hormone) and testosterone from the same precursor molecule. When cortisol demand is chronically elevated — as it is under persistent psychological or physiological stress — the body redirects resources toward cortisol production at the expense of testosterone synthesis. This is known as the cortisol-testosterone axis, and it operates at both the hypothalamic-pituitary level (reducing the LH signal to the testes) and at the testicular level directly.
For many young men in Yorkshire managing high-pressure careers or businesses, this mechanism is a genuinely significant contributor to their hormonal decline — one that often goes unrecognised because stress is so normalised in daily life.
Poor Sleep Quality and Insufficient Sleep Duration

The majority of daily testosterone production occurs during sleep — specifically during deep, slow-wave sleep stages. Studies have shown that even short periods of sleep restriction produce measurable reductions in testosterone. One frequently cited study found that a week of sleeping fewer than five hours per night reduced testosterone in young healthy men by up to 15%.
In a population where poor sleep is endemic — driven by shift work, screen time, late-night habits, and chronic stress — it is unsurprising that testosterone levels are affected. What is less well recognised is that sleep disruption can suppress testosterone to clinically meaningful levels even in otherwise healthy younger men.
Excessive Alcohol Consumption
Chronic alcohol use is a well-established suppressant of testosterone production. Alcohol impairs the function of Leydig cells in the testes — the cells responsible for testosterone synthesis — and disrupts the hypothalamic-pituitary-gonadal (HPG) signalling pathway. Heavy drinking is also associated with elevated oestrogen levels in men, compounding the hormonal imbalance.
This is not a message about occasional drinking. The hormonal impact of moderate, occasional alcohol consumption is minimal. But men who drink heavily and regularly — which, for many working men in Hull and Yorkshire, has become a deeply normalised social pattern — can experience significant testosterone suppression as a result.
Sedentary Lifestyle and Lack of Resistance Training

Physical inactivity contributes to low testosterone through several interconnected mechanisms: it promotes fat accumulation (which increases aromatase activity), reduces anabolic stimulus, and is associated with poorer sleep quality, higher stress, and worse metabolic health. Resistance exercise — particularly compound lifts — is one of the most potent natural stimuli for testosterone production, and its absence removes that stimulus entirely.
For desk-bound men in their twenties and thirties — a rapidly growing demographic across Yorkshire — the combination of prolonged sitting, low physical activity, and rising body fat creates a hormonal environment that is profoundly unsupportive of healthy testosterone production.
Poor Diet and Nutritional Deficiencies
Testosterone synthesis is an energy-intensive process that requires adequate availability of cholesterol, healthy fats, and specific micronutrients. Diets that are highly processed, low in dietary fat, or lacking in key micronutrients create the nutritional conditions for reduced testosterone production.
Deficiencies in zinc, magnesium, and vitamin D are particularly relevant. Zinc is directly involved in testosterone synthesis and the regulation of aromatase. Magnesium affects free testosterone availability. Vitamin D — deficiency of which is exceptionally common in the UK due to limited sun exposure — has been shown in population studies to be strongly correlated with testosterone levels. Correcting genuine deficiencies in these nutrients can meaningfully support hormonal health in men whose diets are inadequate.
Medical Causes of Low Testosterone in Young Men
Beyond lifestyle factors, several medical conditions can cause or contribute to testosterone deficiency in younger men. These are important to identify because some are treatable in ways that go beyond testosterone replacement alone.
Type 2 Diabetes and Insulin Resistance
The relationship between insulin resistance, type 2 diabetes, and testosterone deficiency is bidirectional and well-documented. Insulin resistance impairs Leydig cell function and reduces LH sensitivity, directly suppressing testosterone production. Simultaneously, low testosterone worsens insulin sensitivity and promotes fat accumulation — perpetuating the metabolic dysfunction.
Given the rising prevalence of type 2 diabetes and pre-diabetes in men under 40 across the UK, this is an increasingly significant cause of hypogonadism in younger men. Many men presenting to our Hull clinic with testosterone deficiency also have undiagnosed insulin resistance, which our comprehensive metabolic screening is designed to identify.
Pituitary and Hypothalamic Disorders
Secondary hypogonadism in younger men can result from structural or functional abnormalities affecting the pituitary gland or hypothalamus — the brain regions that control testosterone production via the HPG axis. Causes include pituitary adenomas (benign tumours), hyperprolactinaemia (elevated prolactin levels), haemochromatosis (iron overload), and, less commonly, Kallmann syndrome (a congenital condition affecting GnRH production).
Elevated prolactin is a particularly important and frequently missed cause of secondary hypogonadism in young men. Prolactin directly suppresses LH secretion, reducing the hormonal signal to the testes. A comprehensive hormone panel that includes prolactin measurement — which ours does at Vitalis Luxe Clinic — is essential to detect this.
Medications
Several medications commonly prescribed to younger men can significantly suppress testosterone levels. These include:
- Opioid analgesics (including prescribed codeine, tramadol, and stronger opioids) — opioid-induced androgen deficiency (OPIAD) is well documented and often unrecognised
- Glucocorticoids (including oral and inhaled corticosteroids used for asthma and inflammatory conditions) — suppress the HPG axis with prolonged use
- Some antidepressants and antipsychotics can elevate prolactin and affect hormonal signalling
- Anabolic steroid misuse and subsequent withdrawal suppress the body’s own testosterone production, sometimes for extended periods
- Certain antihypertensives and medications for hair loss (finasteride) — hormonal mechanisms relevant to testosterone and DHT
If you are taking any of these medications and experiencing symptoms of low testosterone, this should be discussed explicitly with your clinician during your assessment.
Genetic and Congenital Conditions
Some younger men with low testosterone have an underlying genetic or congenital condition affecting testicular development or function. Klinefelter syndrome (47,XXY chromosomal pattern) is one of the most common genetic causes of male hypogonadism and is frequently not diagnosed until adulthood. Cryptorchidism (undescended testes in childhood), orchitis (testicular inflammation) following viral infection such as mumps, and previous testicular trauma or surgery can also impair testosterone production in younger men.
Common Causes of Low Testosterone in Young Men: At a Glance
Cause | Type | Modifiable? |
|---|---|---|
Obesity / excess visceral fat | Lifestyle / Metabolic | Yes — weight loss improves T |
Chronic stress / elevated cortisol | Lifestyle / Psychological | Yes — stress management, lifestyle |
Poor sleep/sleep restriction | Lifestyle | Yes — sleep optimisation |
Excessive alcohol consumption | Lifestyle | Yes — reduction improves T |
Sedentary lifestyle | Lifestyle | Yes — resistance training helps |
Nutritional deficiencies (Zn, Mg, Vit D) | Dietary | Yes — dietary improvement or supplementation |
Partially — depends on the cause | Metabolic / Medical | Partially — metabolic management |
Elevated prolactin / pituitary disorder | Medical | Genetic/congenital (e.g. Klinefelter) |
Medications (opioids, glucocorticoids) | Pharmacological | Partially — review with clinician |
Genetic/congenital (e.g.,Klinefelter) | Medical | No — requires clinical management |
Recognising Low Testosterone Symptoms in Younger Men
The symptoms of testosterone deficiency are the same regardless of age — but in younger men, they are more likely to be dismissed, misattributed, or overlooked, both by the men themselves and by healthcare professionals who don’t expect to see hypogonadism in a 28-year-old.
The most common symptoms we see in younger men presenting to our Hull clinic include:
- Persistent, unexplained fatigue — not relieved by rest or adequate sleep
- Low mood, emotional flatness, or depressive symptoms that don’t respond to standard treatment
- Reduced libido — a sustained loss of sex drive that isn’t explained by relationship factors
- Difficulty building or maintaining muscle mass despite consistent training
- Brain fog, poor concentration, or reduced cognitive sharpness
- Increasing body fat, particularly around the abdomen, despite exercise and a reasonable diet
- Reduced motivation and drive across all areas of life — work, relationships, hobbies
- Sleep disturbances — difficulty falling asleep, waking frequently, feeling unrefreshed
A Word on MisdiagnosisThese symptoms in younger men are frequently attributed to clinical depression, burnout, or anxiety — and treated accordingly — while the underlying hormonal cause goes unaddressed. If you have been prescribed antidepressants or anxiety medication and have not experienced the improvement you expected, a testosterone blood test is worth pursuing. Low testosterone can present identically to depression, and treating a hormonal deficiency with antidepressants will not resolve the underlying problem. |
Getting a Proper Diagnosis: What Young Men Should Expect
If you are a younger man concerned about low testosterone, the most important step is a comprehensive blood test — not a single testosterone reading, and not self-diagnosis based on online calculators.
At Vitalis Luxe Clinic in Hull, our assessment for younger men with suspected hypogonadism includes a full hormone panel covering:
- Total testosterone and free testosterone — measured in a morning fasting sample for accuracy
- SHBG (sex hormone-binding globulin) — elevated SHBG can reduce free testosterone even when total levels appear normal
- LH and FSH — to distinguish primary from secondary hypogonadism
- Prolactin — to identify pituitary causes of secondary hypogonadism
- Oestradiol (E2) — to assess aromatase conversion and hormonal balance
- Thyroid function — thyroid disorders can mimic or contribute to testosterone deficiency symptoms
- Full blood count, liver function, HbA1c / fasting glucose — to assess metabolic health and identify insulin resistance
- Vitamin D, zinc, ferritin — to identify relevant nutritional deficiencies
The results are reviewed in the context of your symptoms, health history, medications, and lifestyle — not simply compared to a population reference range. A 25-year-old man with a testosterone of 9 nmol/L and significant symptoms is not well served by being told his result is technically ‘normal’.
Struggling With Low Testosterone Symptoms?
If you’re experiencing fatigue, low libido, brain fog, or reduced performance, it could be more than just stress. Get a professional hormone assessment and personalised treatment plan from our expert team.
Book Your Consultation Call NowTreatment Options for Younger Men With Low Testosterone
The treatment approach for younger men with testosterone deficiency depends on the underlying cause, the severity of deficiency, and, importantly, whether the man wishes to preserve fertility in the near or medium term.
Lifestyle Optimisation — Always the Starting Point
For men whose deficiency is primarily lifestyle-driven — excess body fat, chronic stress, poor sleep, nutritional deficiencies — evidence-based lifestyle modifications can produce meaningful improvements in testosterone and should always be the first intervention. At Vitalis Luxe Clinic, we discuss and support lifestyle optimisation as an integral part of every assessment, regardless of whether TRT is also indicated.
Testosterone Replacement Therapy (TRT)
For younger men with confirmed, clinically significant deficiency — particularly where symptoms are substantially impacting quality of life and lifestyle optimisation has been explored — TRT is a legitimate and effective treatment option. It is not exclusively for older men, and there is no clinical basis for withholding it from younger men who have a confirmed diagnosis and a clinical need.
One important consideration specific to younger men is the effect of TRT on fertility. Exogenous testosterone suppresses the body’s own production of FSH and LH, which in turn reduces sperm production. For men who are not currently trying to conceive but wish to preserve that option, specialist guidance on fertility preservation should form part of the conversation before TRT is commenced.
Alternative Approaches for Fertility Preservation
For younger men with secondary hypogonadism who wish to maintain fertility, alternative treatments such as selective oestrogen receptor modulators (SERMs, e.g. clomiphene) or human chorionic gonadotropin (hCG) injections may stimulate the body’s own testosterone production while preserving sperm production. These are specialist interventions that require careful clinical assessment and monitoring — and are discussed at our Hull clinic where clinically relevant.
Frequently Asked Questions
Can young men in their 20s have low testosterone?
Yes. While testosterone deficiency is more common in older men, it can affect men at any age. Primary hypogonadism (testicular failure) and secondary hypogonadism (pituitary signalling problems) both occur in younger men. Lifestyle factors including obesity, chronic stress, poor sleep, and excessive alcohol consumption, are increasingly significant causes of testosterone deficiency in men under 40.
What are the most common causes of low testosterone in young males?
The most common causes in younger men include excess visceral body fat (through the aromatase conversion mechanism), chronic psychological or physiological stress, poor sleep quality and duration, excessive alcohol consumption, insulin resistance, and pituitary disorders including elevated prolactin. Nutritional deficiencies — particularly vitamin D, zinc, and magnesium — can also contribute meaningfully in some individuals.
How do I know if I have low testosterone as a young man?
Symptoms including persistent fatigue, low mood, reduced libido, difficulty building muscle, brain fog, and increasing abdominal body fat occurring together are strong indicators — but symptoms alone cannot confirm the diagnosis. A comprehensive morning blood test covering total testosterone, free testosterone, SHBG, LH, FSH, and supporting markers is required. At Vitalis Luxe Clinic in Hull, we offer this full assessment for men across Yorkshire.
Is low testosterone in young men treatable?
Yes. Treatment depends on the underlying cause. Where lifestyle factors are the primary driver, evidence-based changes to sleep, exercise, diet, and stress management can meaningfully improve testosterone levels. For men with clinically confirmed deficiency that doesn’t respond to lifestyle optimisation, TRT is an effective, evidence-based treatment. The specific approach is determined through a comprehensive clinical assessment.
Can low testosterone in young men affect fertility?
Yes. Testosterone deficiency in younger men — particularly secondary hypogonadism affecting LH and FSH signalling — can impair sperm production and reduce fertility. This is an important consideration when discussing treatment options, as TRT itself also suppresses sperm production. Men who wish to preserve fertility should discuss specialist options at their consultation.
Is it worth seeing a TRT clinic in Hull if I’m under 35?
Absolutely. There is no age threshold below which testosterone deficiency should be dismissed. If you are experiencing symptoms that affect your quality of life, work, relationships, and physical health, you deserve a thorough investigation, regardless of your age. At Vitalis Luxe Clinic, we assess men of all ages and take every presentation seriously.
Will my GP test my testosterone if I’m young?
GPs can request testosterone testing, but younger men may find it more difficult to access a thorough investigation on the NHS — particularly if their result falls within the broad population reference range while still being symptomatic. A specialist private clinic like Vitalis Luxe Clinic in Hull offers more comprehensive testing, a broader interpretation framework, and a wider range of treatment options tailored to the needs of younger men.
How quickly can testosterone levels improve with lifestyle changes?
Meaningful improvement in testosterone levels from lifestyle changes typically takes 8–16 weeks of consistent effort. The most impactful interventions — significant fat loss, consistent resistance training, sleep optimisation, and stress reduction — need time to produce measurable hormonal changes. Regular blood testing allows us to track progress and determine whether clinical intervention is additionally required.